The 2025 Life Care Planning Summit, held on May 16th and 17th in Minneapolis, Minnesota offered a unique and inspiring forum for professionals from diverse primary professional disciplines including nursing, rehabilitation counseling and other rehabilitation professions to unite in the advancement of the specialized practice of life care planning. This gathering provided an invaluable platform for exchanging ideas, fostering professional growth, and promoting best practices amid the rapidly evolving landscapes of healthcare, rehabilitation and the legal system. It spotlighted the leaders shaping educational programs, professional organizations, and certification standards within the field. Through rich interdisciplinary dialogue, participants generated fresh insights and renewed energy, collectively shaping the future of life care planning.
Next, the Summit focused on the organization and refinement of the Consensus and Majority Statements (Johnson et al., 2018). The statements are guiding principles generated through expert collaboration over multiple decades and serve as one of the foundations for life care planning practice. The statements embody the life care planner’s commitment to reliable and valid development of objective, defensible, and client/evaluee-centered life care plans. Reorganizing these statements will further aid the practicing life care planner’s focus on the most relevant and timely guidance.
The 2025 Summit utilized reliable and acceptable methodologies, consistent with those of prior Summits, to achieve the outlined objectives. A mixed methodology was used combining Nominal Group Technique (NGT) (Delbecq et al., 1975) and Audience Response System (ARS) for Real Time Voting (RTV) (Burnstein & Lederman, 2006). Both ARS and RTV were previously used in the 2010 Summit and the 2025 Summit utilized Mentimeter, an online platform that allows for integration of real time data collection into presentations. The platform allowed participants to answer questions using personal electronic devices and populated the data in real time for participants to view the outcome. Over the course of the 2025 Summit, Mentimeter was used to collect data in various formats including questions with word cloud and free response answers, multiple choice trivia questions, and real time voting with a pre-set selection of choices. As reflected in this publication, the 2025 Life Care Planning Summit stands as a testament to the field’s collaborative spirit and unwavering dedication to meeting the complex needs of individuals and families navigating challenging health journeys.
The History and Background of the Life Care Planning Summit
Attendees were briefed on this history of life care planning summits. For a more comprehensive history, see previous summit-related publications in Journal of Life Care Planning, volumes 16(4), 17(3), and 21(1).
Since 2000, life care planners have relied upon the outcomes of the life care planning summits in their daily work. These published results have culminated in the Consensus and Majority Statements (Johnson et al., 2018), which are updated regularly and published in the Journal of Life Care Planning. The works of Johnson and Preston (2012), Johnson (2015), and Johnson et al. (2018) have served as guiding principles for life care planners. Life care planning summit proceedings are developed by life care planners specifically for other life care planners and focus on life care planning practices. Familiarity with the results of these summits, including the publication of Consensus and Majority Statements (Johnson et al., 2018), is crucial for practitioners.
Summits have ensured that life care planners sustain professionalism and confirm that we are not paint by number scribes. They follow the long-standing tenets and methodology consistent with the multidisciplinary aspect of life care planning. These have been reassuringly affirmed in state and federal court decisions and jurisdictions, and adopted by other venues (e.g. Medicare-Set-Aside, family planning, trusts, catastrophic healthcare reserves, workers’ compensation claims, and others) (Albee et al., 2017).
Since its inception, it has been regularly recommended that practitioners take a vested interest in the future of life care planning and actively participate in summits to address emerging issues affecting life care plans, the process of life care planning, and the role of life care planners. There have now been 13 Life Care Planning Summits held throughout the United States and Canada. A brief history of these events is summarized below.
| YEAR |
DATE |
LOCATION |
FOCUS |
COMMENT |
Statements |
| 2000 |
April 12 |
Dallas, TX |
Professional preparation; Basic tenets and procedures for
completing life care plans; |
The first Summit was sponsored and endorsed by the International Association of Rehabilitation Professionals (IARP), the |
28 added |
|
|
|
Ethics; Reliability and validity of the life care plan; Information dissemination. |
International Academy of Life Care Planners (IALCP),
Intelicus/University of Florida and the Commission on Disability Examiner Certification (CDEC). In addition, the American Association of Legal Nurse Consultants (AALNC) and the Case Management Society of America (CMSA) participated. |
|
| 2002 |
May 19 |
Chicago, IL |
Scope of practice; Skills;
Ethics; Professional development; Methodology; Functions; Future of life care planning. |
This Summit focused on the emergence of the specialty practice and the need for Standards of Practice, and future thinking regarding development, methodology and ethics. |
21 added |
| 2004 |
April 24 and 25 |
Atlanta, GA |
Certification Process;
CLCP® examination and continuing education credits; Future research in life care planning; CLCP mentoring program; Standards of practice for life care planners. |
First 2-day Summit Continuing discussion regarding the emergence of the Standards of Practice and focus on the CLCP certification |
30 added |
| 2006 |
May 6 and 7 |
Chicago, IL |
A panel of representatives of the IALCP, CHCC, and the Foundation for Life Care Planning Research (FLCPR) discussed trends and plans for the future of life care planning and each represented organization had an opportunity to provide input. |
First Panel (Town Hall) Approach |
0 added |
| 2008 |
May 15 and 16 |
Los Angeles, CA |
Visions for the future of life care planning: Identifying controversial aspects of plans created by various professional disciplines; Developing unity in the specialty practice: Standards of practice shaping the role and function of life care planning;
Best practices: Methodology issues in data collection; Best practices: Methodology issues in creating admissible life care plans;
Research: Priorities, needs, and practical applications in day- to-day practice; Professional business issues: Risks and benefits of databases, templates, and software. |
|
9 added |
| 2010 |
April 17 and 18 |
Atlanta, GA |
Topic 1: Best Practices for Establishing Foundation for Necessity: Boundaries for Decision Making; Topic 2: Best Practices for Determining Sources of Attendant Care in the Home;
Topic 3: Review of Consensus Statements, Majority-View Statements and Results of Life Care Planning Summits 2000 – 2008. |
Technology was first utilized to gather input from attendees in Real Time Voting. |
10 added and one deleted as no longer relevant |
| 2011 |
June 3 and 4 |
Toronto, Canada |
This was a replication of the first Summit to ensure the specialty practice was consistent internationally, although jurisdictional requirements may change. |
|
|
| 2012 |
May 5 and 6 |
Dallas, TX |
This Summit brought together the IALCP, the Foundation for Life Care Planning Research (FLCPR), the International Commission on Healthcare Certification (ICHCC) and the American Association of Nurse Life Care Planners (AANLCP) to begin a collegial dialogue between the various entities promoting life care planning.
Additionally, the topics of ethics and costing were further explored. |
The 2012 Summit provided the 98th and 99th Consensus and Majority Statements as summarized in the Journal of Life Care Planning (JLCP) Volume 11, No. 1 (Preston and
Johnson, 2012).
Following the 2012 Summit, Karen Preston took the lead in a task force which reviewed and revised the IALCP Standards of Practice with the aid of the community of life care planners. This was completed and published in the Standards of Practice for Life Care Planners, Third Edition. |
2 added |
| 2015 |
September 18 |
Scottsdale, AZ |
Best Practices for Business and Best Practices for Transparency were the main topics for the 2015 Summit. Topics discussed in the breakout sessions were: Best Practice in Business of Life Care Planners and Best Practice in Transparency for Life Care Planners. |
This one-day Summit was a full day with a working lunch, including an ethics presentation by Dr. Christine Reid, followed by updates from the IALCP, FLCPR,
American Association of Nurse Life Care Planners (AANLCP), Certified Nurse Life Care Planners (CNLCP) Certification Board, and the International Commission on Health Care Certification (ICHCC). |
3 added |
| 2017 |
May 19 and 20 |
Denver, CO |
The goal was to further define “associated costs” with education and discussion on how costs are derived and appropriate ways to determine and utilize collateral sources. |
As a group, attendees compiled 29 different venues in which a life care plan may be utilized.
Additional consensus:
“A comprehensive and systematic review of the existing 102 statements through a multi-association process to determine if they are still appropriate and relevant is needed.”
“Life care planners shall develop a position statement (white paper) regarding the presentation of charges and/or costs presented in the life care plan that provides guidance to life care planners for the variety of uses and jurisdictional requirements encountered by life care planners. The paper must take into consideration that “associated costs” are referenced in the definition of a life care plan, and ensure the current geographically relevant monetary charges for a good and service in the life care plan.”
There was a consensus to reaffirm other past consensus and majority statements: #98, #86,
#82 and #79 were all reaffirmed by the 2017 Summit proceedings.
“In the future review of the statements, it will be necessary to look closely at #56 and consider the definition of “integrity” (applicability, relevance and the obligation of the life care planner to know the integrity of our data versus only the sources of data).” |
0 added |
| 2022 |
May 13 and 14 |
Dallas, TX |
Topic of Summit: Costing techniques, survey results, and development of a framework in support of the life care planning specialty. |
Utilization of Top Hat technology |
Costing Framework Committee was created. |
| 2025 |
May 16 and 17 |
Minneapolis, MN |
Aligning for Consensus 2025: Past Foundations to Future Needs
Topics:
Distinguish between the different life care planning educational programs, organizations, and certification programs and their benefits and challenges.
•Identify the gaps we have in the field of life care planning that need solutions.
•Analyze the current list of Consensus Statements and how they apply to widely accepted life care planning practice.
•Evaluate the relevancy of individual Consensus Statements to provide a clearer basis for life care planning opinions |
Utilization of Mentimeter Real Time Voting |
Consensus Statements were reviewed, analyzed, and categorized by a Work Group and then by attendees. The outcome was published separately. However, of the 96 prior
statements, 12 remained relevant to the life care planner, not published elsewhere; 41 were relevant to the life care planner and published elsewhere, 15 statements were applicable and advisory to life care planning educational programs, certifying bodies, associations and organizations; 13 statements were added to the three previously deleted and considered historically no longer valid; with 15 statements, while still relevant and applicable to the life care planner were recommended to be under further review. |
Demographics
During the first day of the 2025 Summit, a series of questions regarding relevant demographic background information of the participants was asked using the ARS, and data was collected and presented via RTV to allow the participants to familiarize themselves the other attendees in the room. The questions were as follows:
-
What is your primary profession?
-
What certifications pertaining to Life Care Planning do you hold?
-
Which professional associations are you a member of to support your life care planning practice?
-
In which state/province do you live?
-
How many years of experience do you have preparing Life Care Plans?
-
How many Summits have you attended (including this one)?
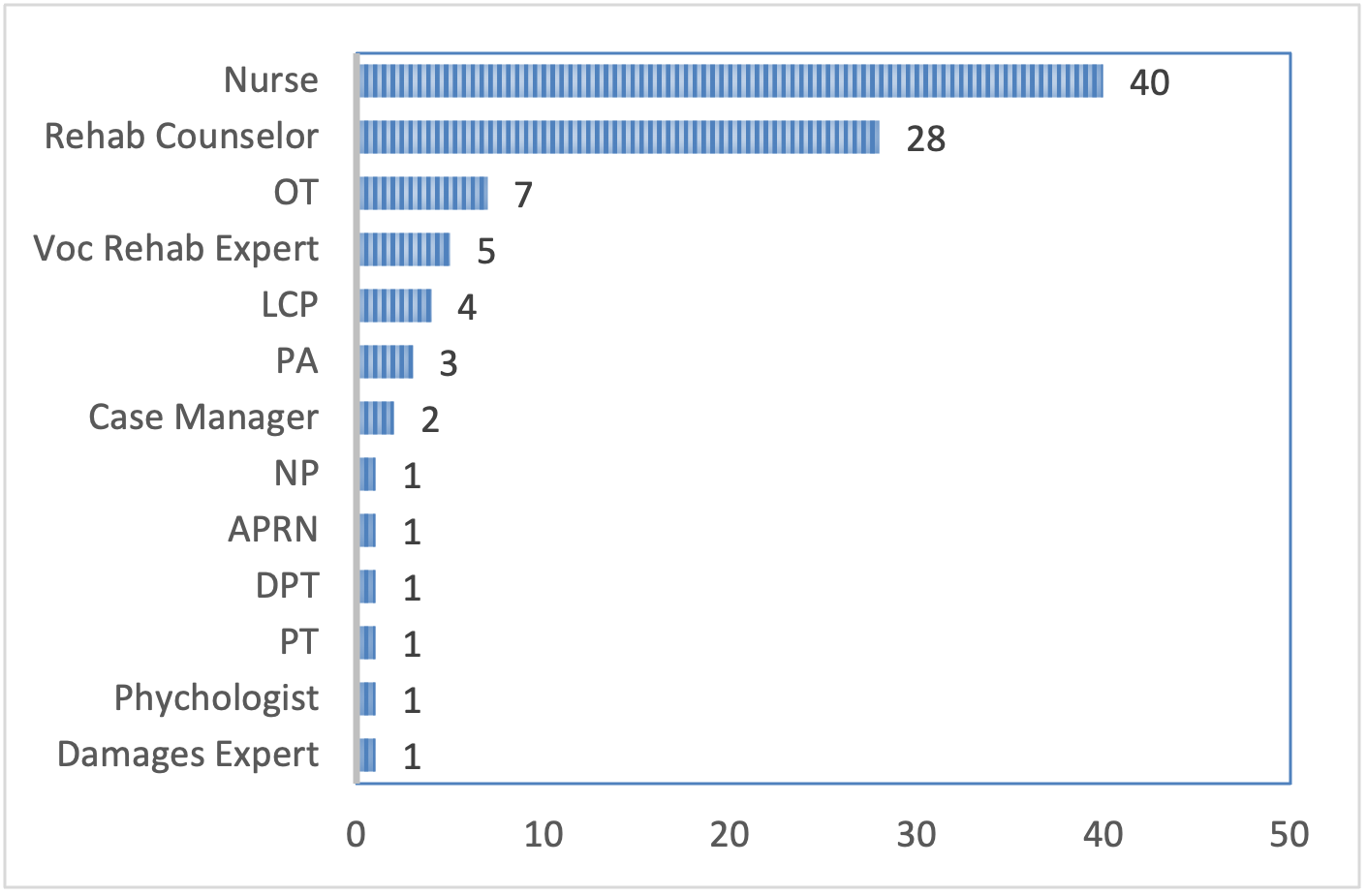
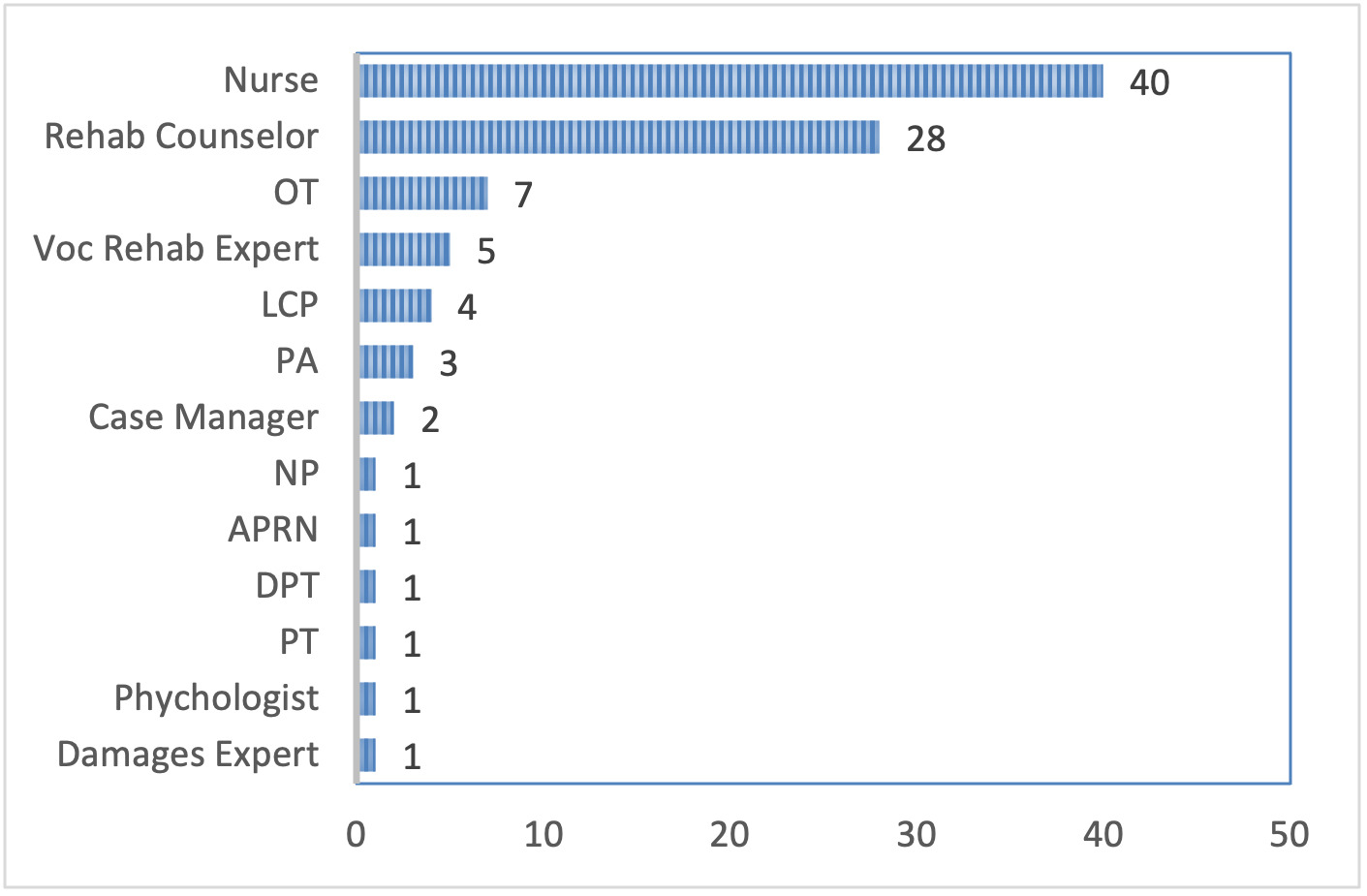
The 2025 Summit attendees self-identified 13 unique primary professions including 42.1% nurses, 29.5% rehabilitation counselors, 7.4% occupational therapists, 5.3% vocational rehabilitation experts, 4.2% life care planners, 3.2% physician assistants, 2.1% case managers, 1.1% nurse practitioners, 1.1% advanced practice registered nurses, 1.1% doctors of physical therapy, 1.1% physical therapists, 1.1% psychologists, and 1.1% damages experts.
Question 1: What is your Primary Profession?
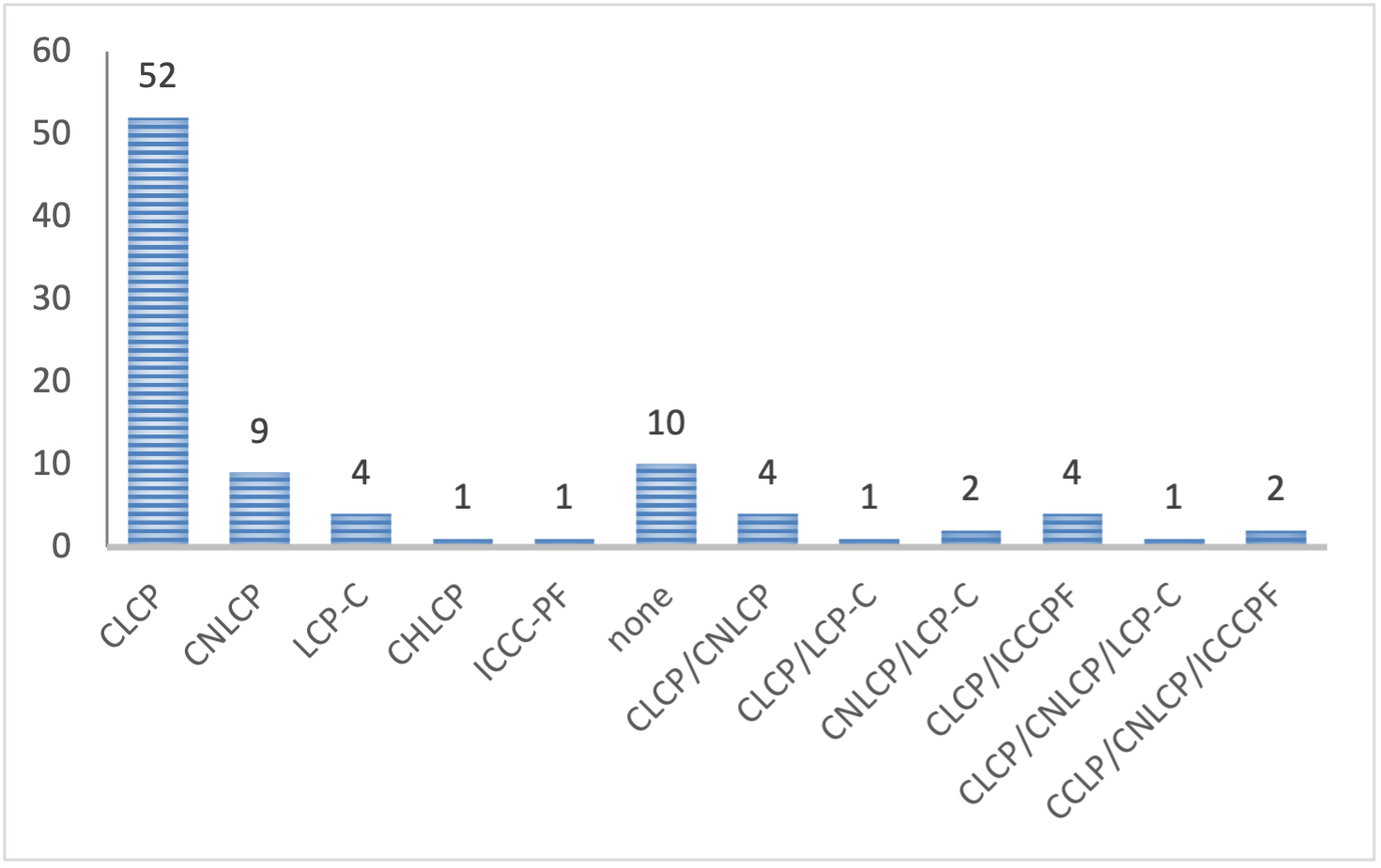
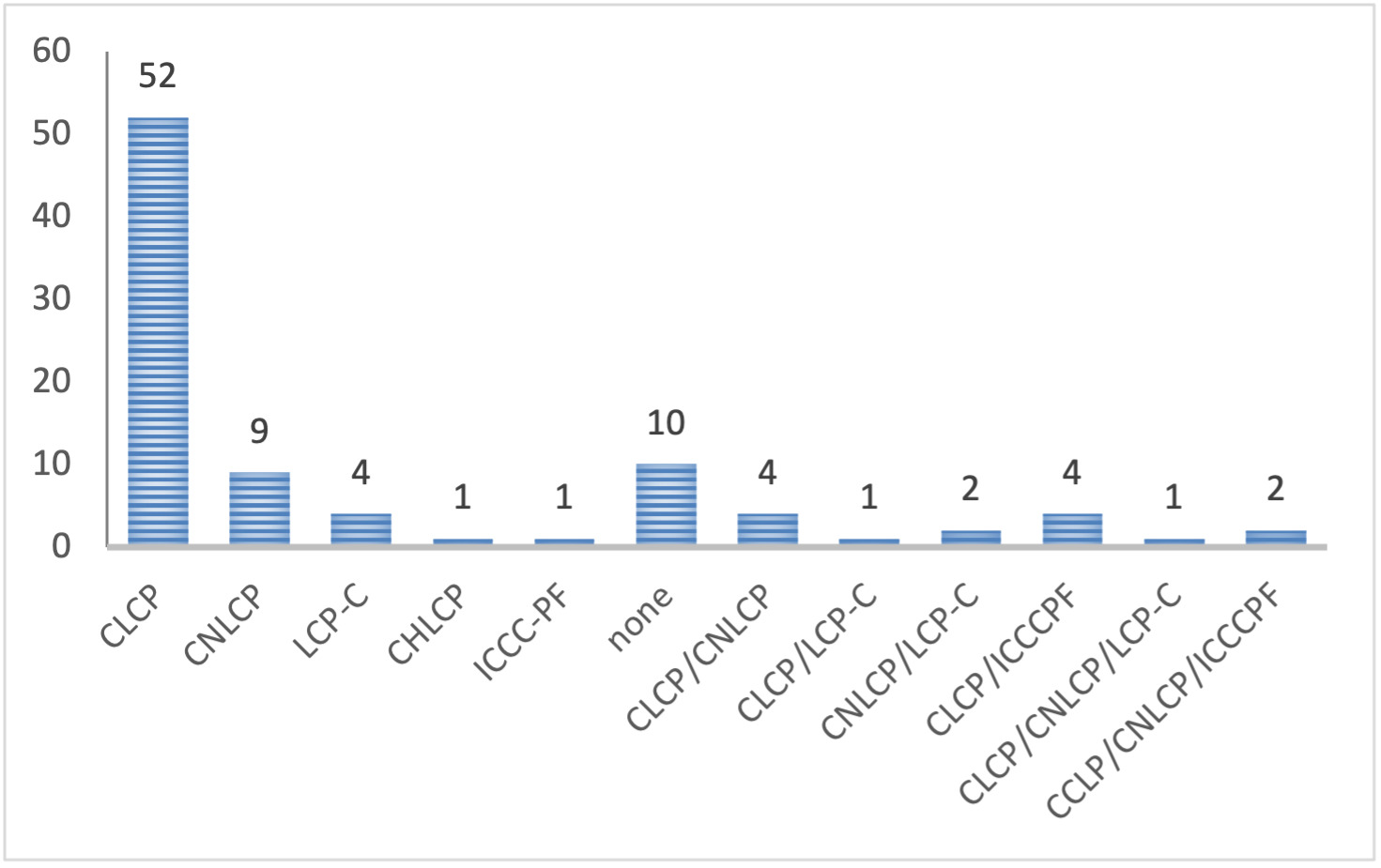
Of the attendees, 89% of attendees self-reported at least one life care planning specific certification, while 11% reported holding none. Of those with a life care planning specific certification, 73.6% held a single certification, 12.1% held two certifications, and 3.3% held three certifications. Of individuals with a single certification, the most common certification was the CLCP with 57.1% of single certification holders having a CLCP followed by CNLCP 9.9%, FIG LCP-C 4.4%, CHLCP 1.1% and ICCC-PF 1.1%. Upon individuals with multiple certifications, combinations of certifications included CLCP/CNLCP, CLCP/FIG LCP-C, CLCP/ICCC-PF, CLCP/CNLCP/FIG LCP-C, and CLCP/CNLCP/ICCC-PF. Alternative certifications attendees held that supported their life care planning practice included CRRN, CRC, CDMS, CCM and ABVE-D.
Question 2: What Certifications Pertaining to Life Care Planning do You Hold?
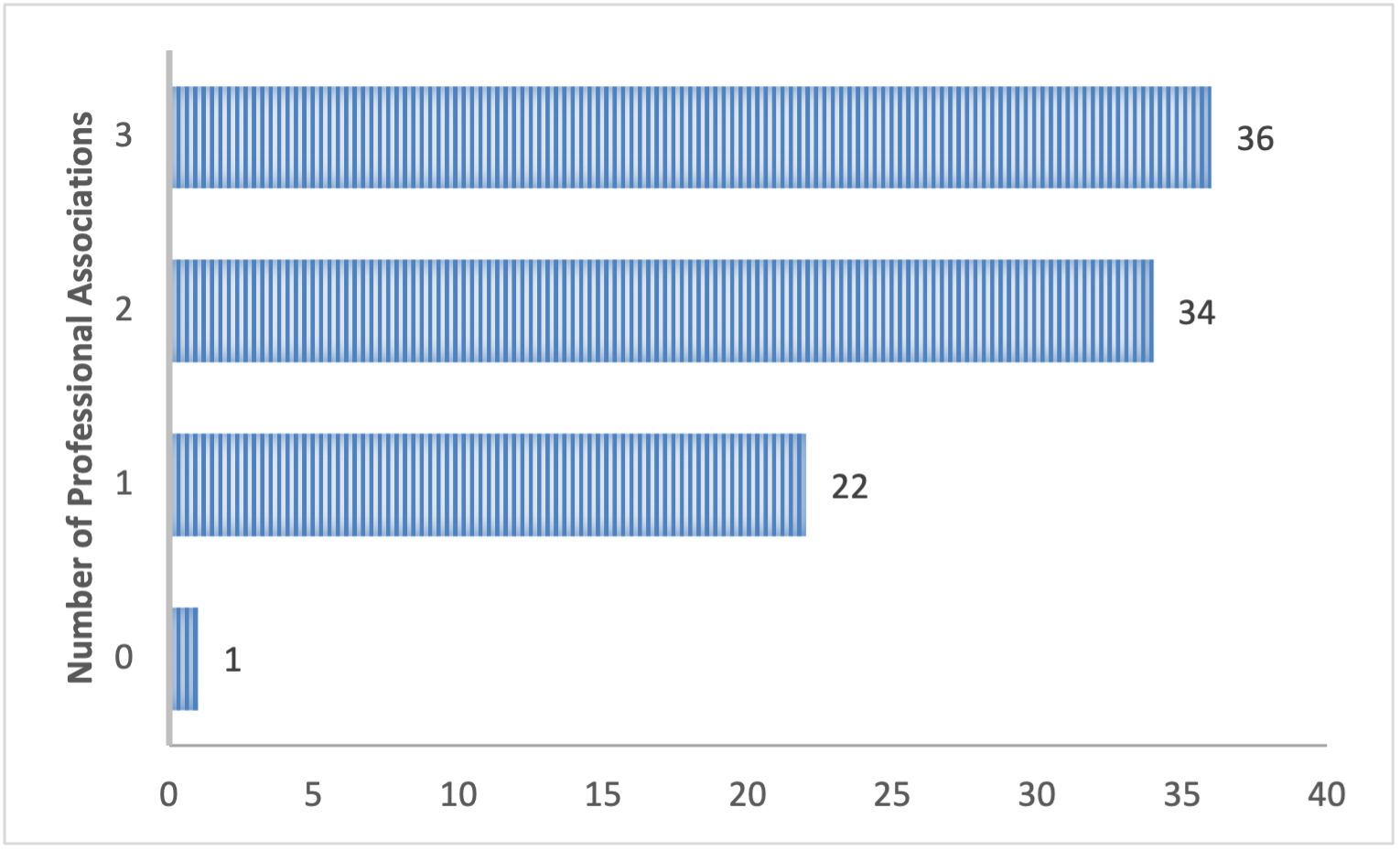
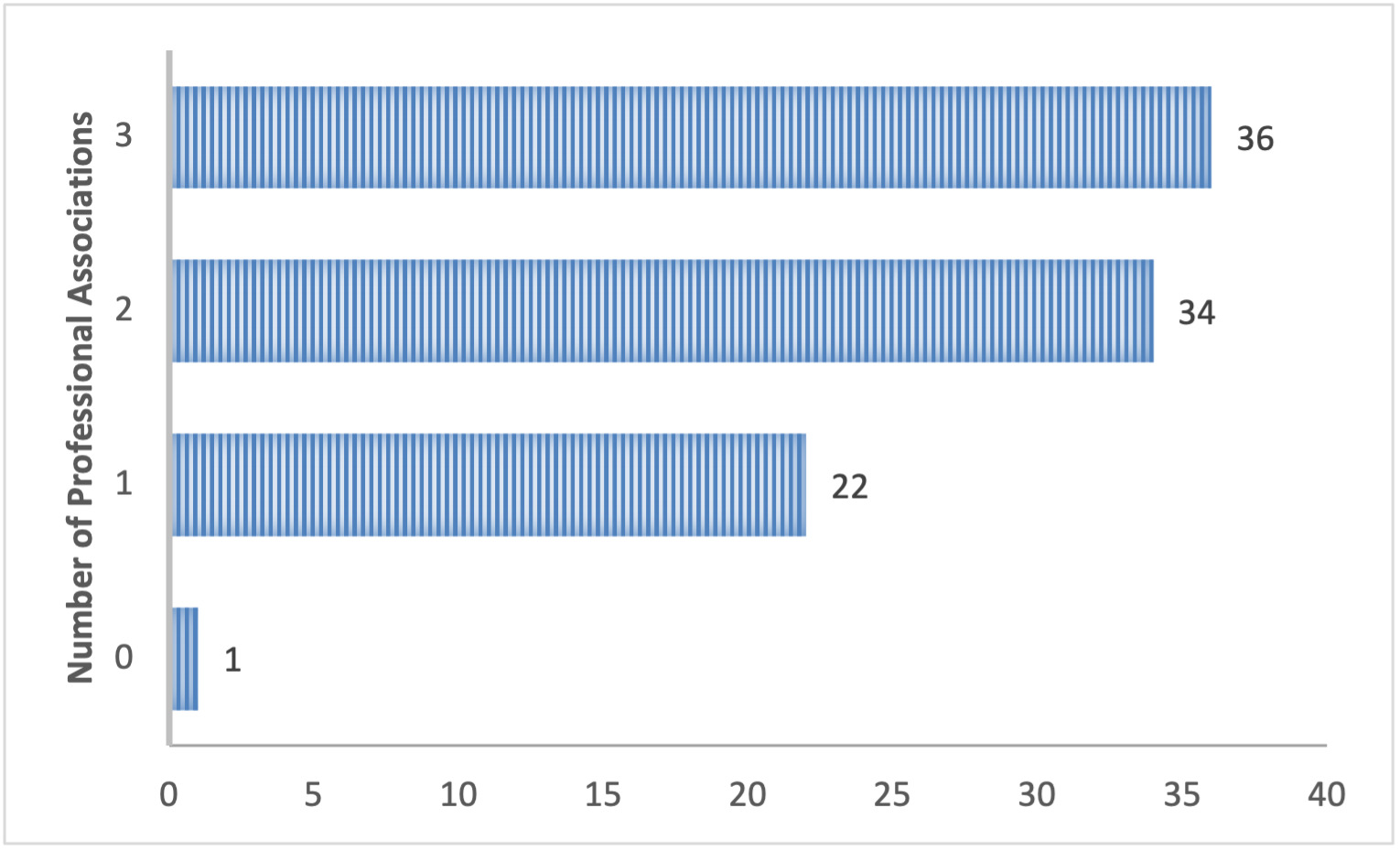
Attendees reported being involved in up to four professional organizations to support their life care planning practice with 1.1% being a member of no organizations, 23.7% being a member of one organization, 36.6% being a member of two organizations, and 38.7% being a member of three organizations. Organizations listed by participants included the International Association of Rehab Professionals (IARP), the International Academy of Life Care Planners (IALCP), American Association of Nurse Life Care Planners (AANLCP), Association of Certified Life Care Planners (A-CLCP), Association of Rehabilitation Nurses (ARN), Case Management Society of America (CMSA), American Academy of Professional Coders (AAPC), American Association of Legal Nurse Consultants (AALNC), North American Nursing Diagnosis Association International (NANDA-I), American Board of Vocational Experts (ABVE), College of Vocational Rehabilitation Professionals (CVRP), American Occupational Therapy Association (AOTA), and American Rehabilitation Economics Association (AREA).
Question 3: Which Professional Associations Are You a Member of to Support Your Life Care Planning Practice?
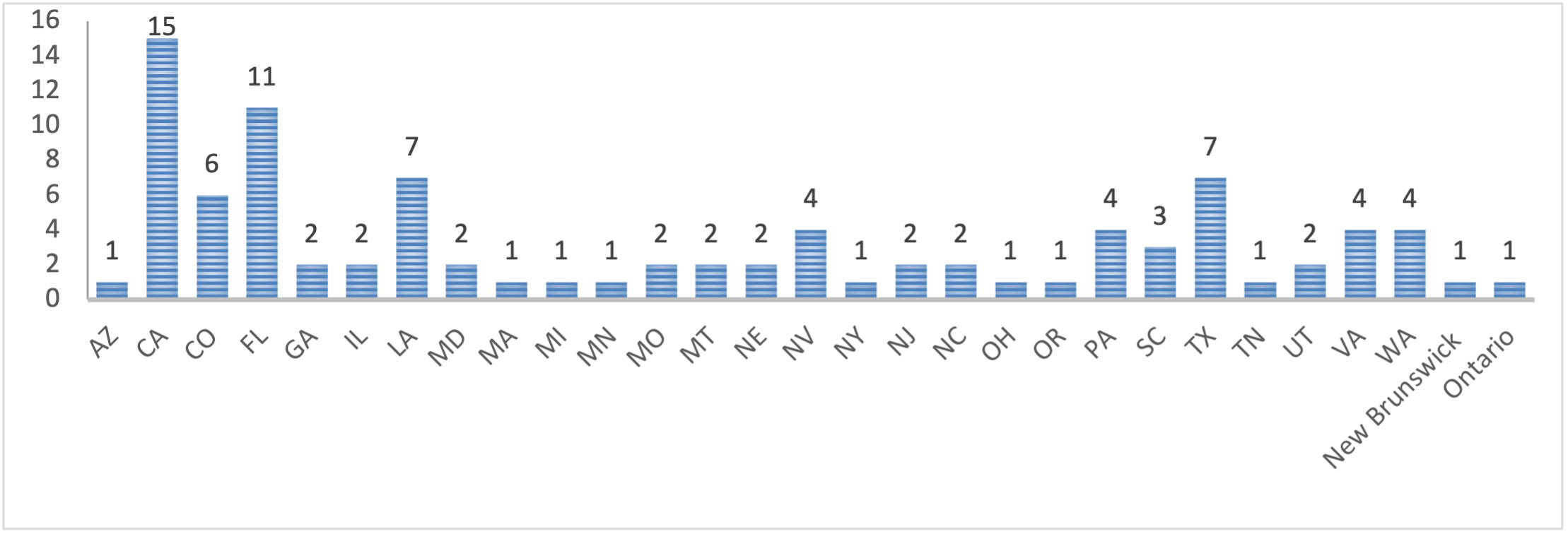
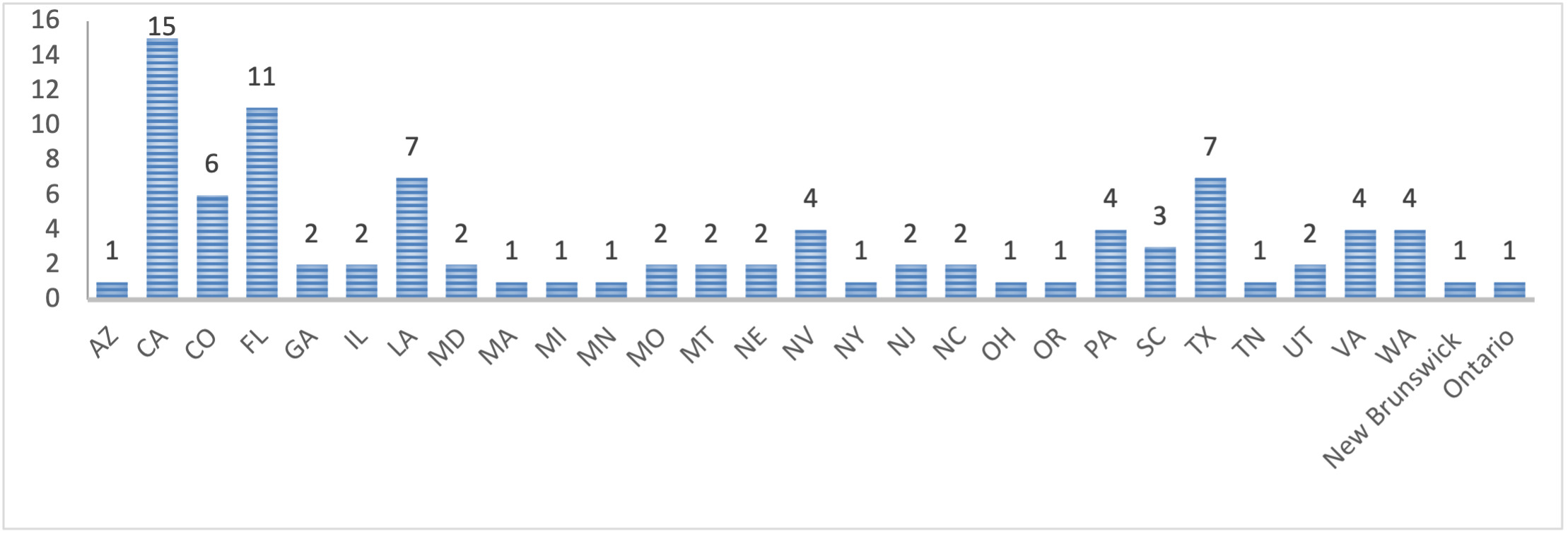
Twenty-seven states and two provinces were represented including Arizona, California, Colorado, Florida, Georgia, Illinois, Louisiana, Maryland, Massachusetts, Michigan, Minneapolis, Missouri, Montana, Nebraska, Nevada, New York, New Jersey, North Carolina, Ohio, Oregon, Pennsylvania, South Carolina, Texas, Tennessee, Utah, Virginia, Washington, New Brunswick, and Ontario.
Question 4: In Which State/Province Do You Live?
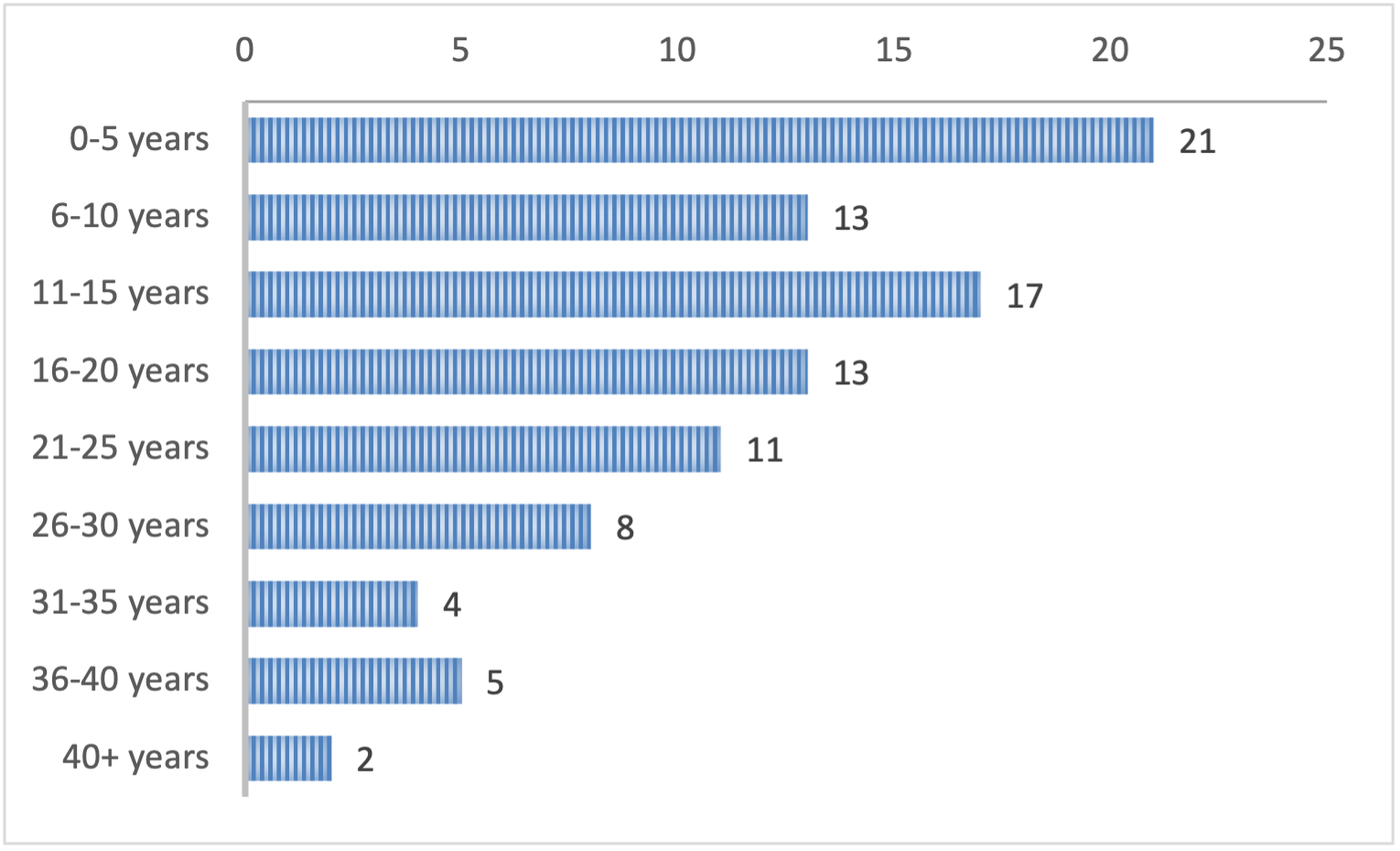
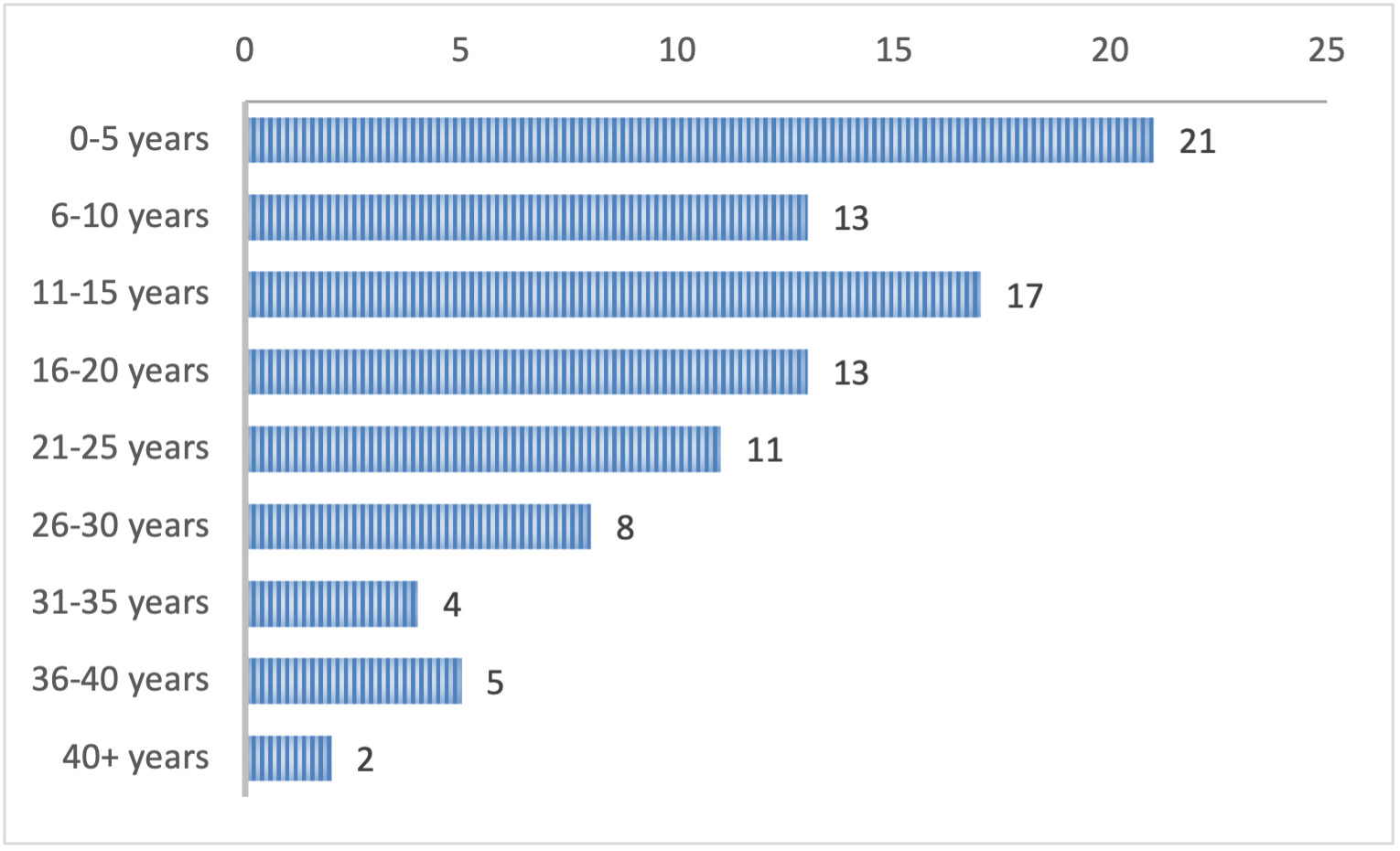
Attendees reported 0-43 years of experience preparing life care plans including 22.3% with 0-5 years of experience, 13.8% with 6-10 years, 18.1% with 11-15 years, 13.8% with 16-20 years, 11.7% with 21-25 years, 8.5% with 26-30 years, 4.3% with 31-35 years, 5.3% with 36-40 years, and 2.1% with greater than 40 years of experience.
Question 5: How Many Years of Experience do You Have Preparing Life Care Plans?
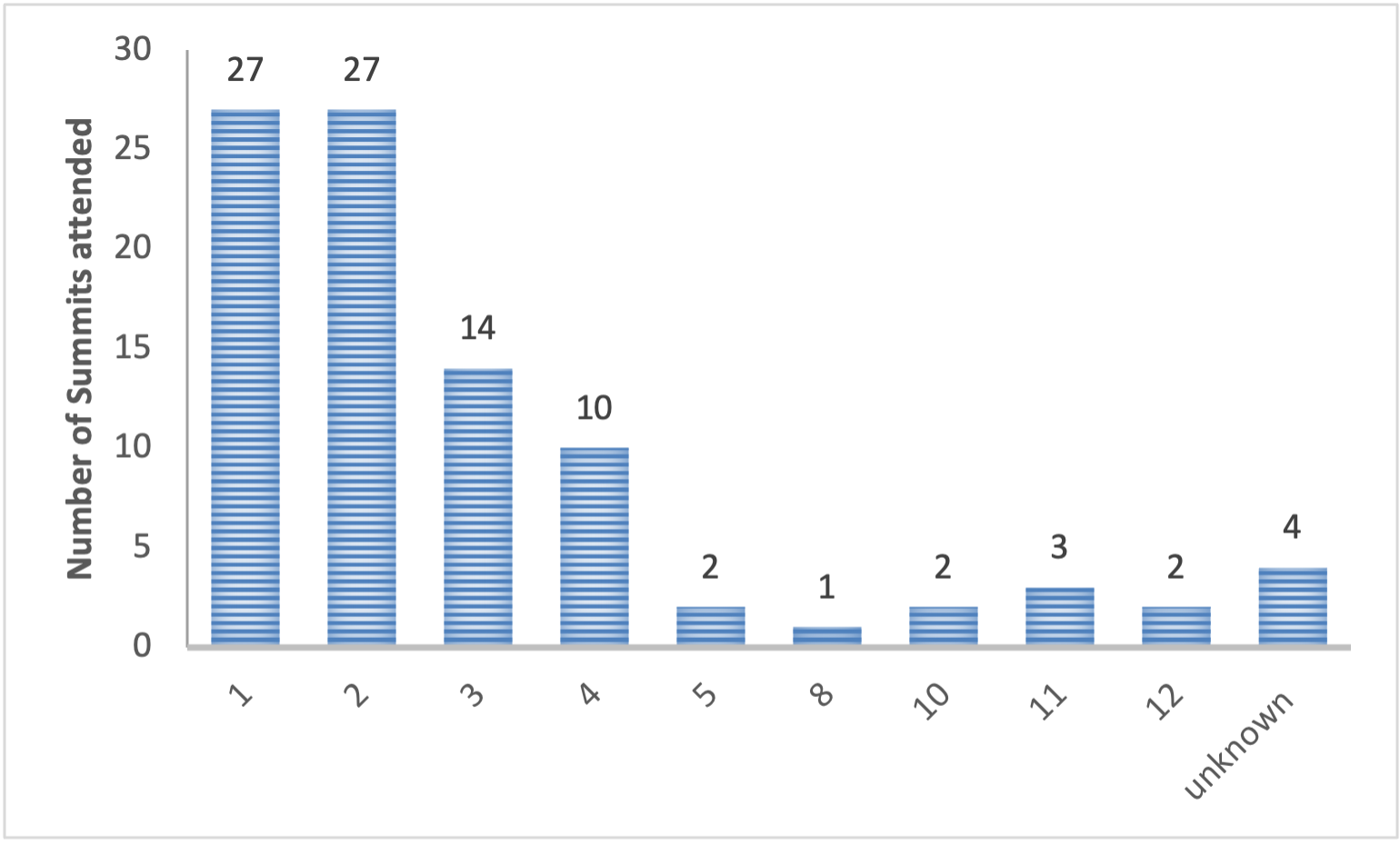
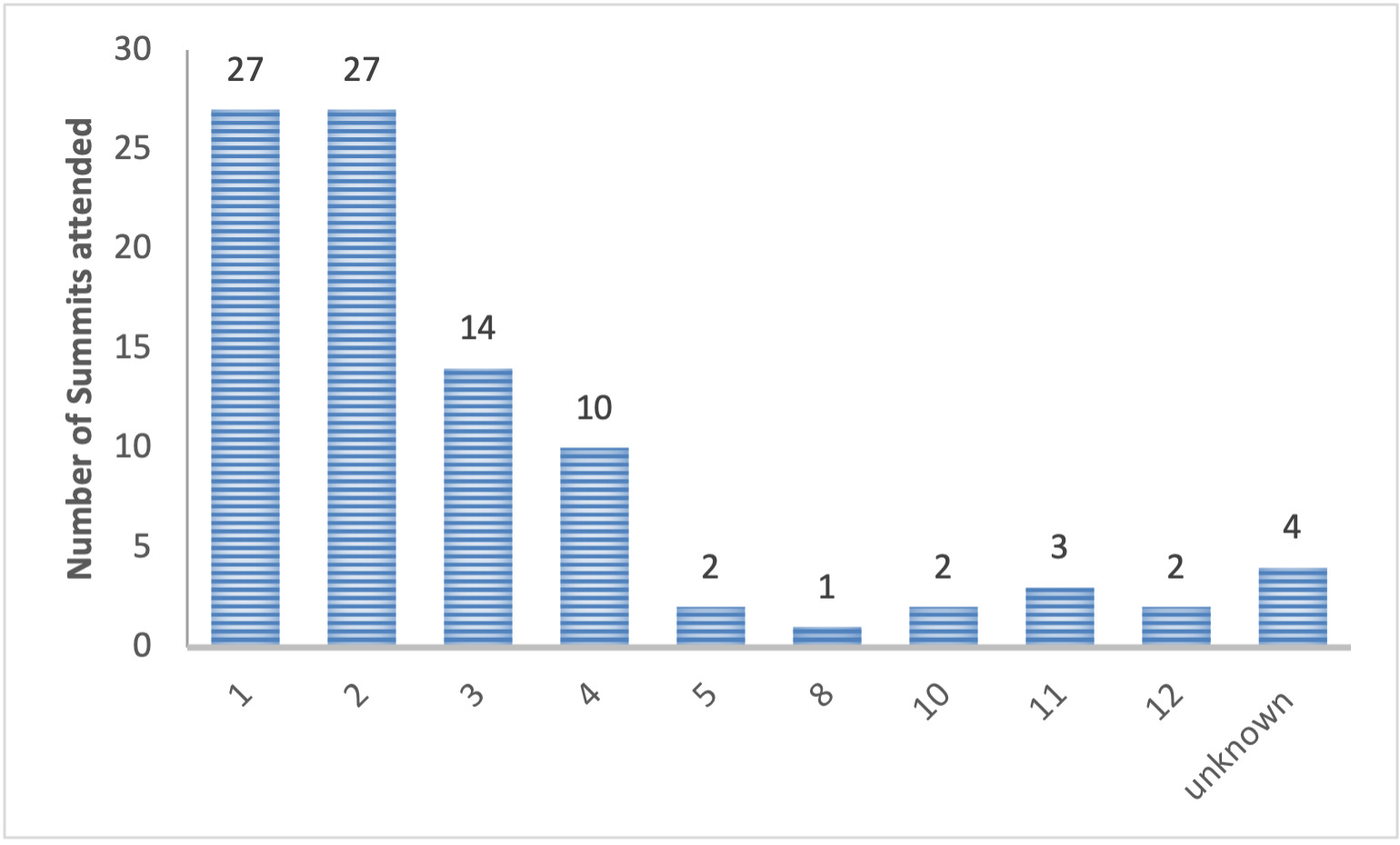
When asked how many summits they had attended, including the 2025 Summit, 29.3% reported that they were first time attendees. Amongst the remaining attendees, number of summits attended ranged from two to 12 with 29.3% having attended two, 15.2% having attended three, 10.9% having attended four, 2.2% having attended five, 1.1% having attended eight, 2.2% having attended 10, 3.3% having attended 11, 2.2% having attended 12, and 4.3% having attended an unknown number of summits.
Question 6: How Many Summits Have You Attended (Including This One)?
Part 1: Breakout Sessions
All known life care planning entities who oversee education programs, certifications, professional associations, and research organizations were invited to participate in the 2025 Summit and educate the attendees on their mission, goals, and specific details about their program. Questions were developed by the 2025 Life Care Planning Summit planning committee, and interviews were conducted as short question-and-answer style pre-recorded presentations.
On day one of the Summit, the pre-recorded presentations were divided into sessions by category (Educational Programs, Professional Associations/Research Organizations, Certifying Bodies) and played for the attendees. Following each session, the attendees divided into their assigned breakout rooms to discuss the information provided in the presentations utilizing a modified nominal group technique methodology to ensure all attendees had a voice. Participants were asked to answer using the ARS and RTV, three specific questions: (1) What are the strengths? (2) What are the concerns? (3) What do we need? The data for each question was collected via free-form answer using Mentimeter and compiled to identify the most recorded responses. The outcomes of the presentation and discussion groups were as follows:
Education Programs
| What is the name of your program? |
AAACEU
Certified Life Care Planner (CLCP) Training Program |
FIG
Education
Certification Class in Life Care Planning |
Kelynco
Nurse Life Care Planning Course |
Institute of Rehabilitation and Education Training (IRET)
Life Care Planning Pre- Certification Program |
Southwest Florida Training Institute
Life Care Planning Bootcamp |
Thomas Jefferson University
Life Care Planning Graduate Certificate |
| What is received at the end of your program? |
A series of certificates to show completion of the requirements put out by ICHCC for the CLCP. |
A certificate of completion. |
120 contact hours approved by ANCC |
Certificates of completion for the modules and work sample. |
A certificate of completion. |
9-credit advanced graduate certificate. |
| What are the requirements for entry into your program? |
There are no requirements, everyone is welcome. |
Open to everyone. |
A nursing degree. Experience in case management or rehabilitation is preferred |
No specific requirements. |
Students are required to meet eligibility requirement s for the CLCP set by the ICHCC. |
BS or BA in health or social sciences plus whatever the minimum requirement is in your primary discipline. |
| What are the core teaching topics of your program? (topics, hours, core literature). |
120 hours made up of 7 modules and a sample LCP.
Course materials include articles, journal papers, and pre-recorded videos. |
120 hours broken into 24 lessons, 5 hours each. Each lesson has a recorded presentation, readings, and a homework assignment.
Cover plan development, nursing, case management, rehabilitation process, common diagnoses seen in life care planning, and how to be a successful expert. |
120 hours.
The foundation of the course is the nursing process at its core.
Course materials include printed books and online webinars. |
Six modules, about 20 hours each.
Background on life care planning, medical and psychosocial aspects of different disabilities and how to apply them to life care plan development, and the forensic aspects of life care planning.
Also includes mock trial and deposition experience. |
120 hours.
Course materials include textbooks, JLCP articles, RehabPro articles, and other peer reviewed literature. |
Intro to life care planning and the practice standards, intro to the most common conditions seen in life care planning, costing, and forensic litigation.
Has a mock trial during the forensic course. |
| Is your educational program affiliated with a university or higher education program? |
No |
No. |
No |
No longer directly affiliated. |
No |
Yes. |
Does your educational program have a peer review
requirement? |
Yes. |
Yes. |
Yes. All course work is peer reviewed. |
Yes. |
Yes. |
Yes. |
| What is the time investment and the total cost for your educational program? |
Costs are $500 per module or $3,000 as a 7-module bundle, plus $299 for the peer-review of the sample LCP.
Total time required depends on the student. Most take several months to complete. |
Cost is $3,999 for all materials and modules.
Course is 120 hours with a goal of completing within 6 months. |
Costs are $600 per online module (5 total) and
$750 for the virtual/onsite module,
$3,750 total. This cost does not include the peer review life care plan which is an additional $350.
Students have 90 days to complete each course after registering.
Try to keep students on track to complete within a year. |
Costs start at $3,500.
It depends on the individual. Usually 2-6 months. |
Costs are $599 per course or $2,750 for the 5- course bundle plus
$250 for the peer-review of the sample LCP. |
Costs are $600 per credit hour for 9 credit hours, $5,400 total.
Course runs from September to August and follows the graduate school semester. |
Do you offer continuing education for life care planning certification(s
)? If, so please describe which CEUs you offer. |
Yes. They have 66 courses approved for CEUs for the CLCP (including ethics) offered individually or in bundles. |
Yes. Each individual lesson can be taken as continuing education for 5 CEUs. Also offer onsite retreats where topics are looked at more in- depth.
CEUs options are also approved for nursing contact hours. |
No |
No |
None at this time. |
No. |
| What challenges do you face in leading an education program? |
Staying on the forefront and on top of research and developments to ensure they are delivering relevant coursework. |
Keeping up to date with current trends in life care planning and keeping the educational content up to date, maintaining a united front in the field across all the different primary professions, and supporting graduates. |
Adapting to all student needs and ensuring that everyone’s learning needs are met. |
Staying current on topics.
Evolving certificate options. Maintaining experience in the field to provide instruction. |
Not having enough time to market. |
Running the program within the graduate school adds a barrier to completion time. Also adds a costs barrier because costs are set by the university. |
The break out groups identified the top strengths of the current educational programs to include accessibility and flexibility, variety of available options, and affordability. The top concerns included lack of available mentorship, lack of consistency among educational programs, and the quality of education provided. When asked what the life care planning community needs from their education programs to rectify concerns and improve the education for current and future life care planners, the top answers included increased mentorship and continued support following completion, more in depth education and training on coding and costing for the life care plan, and increased consistency and collaboration among educational programs.
Certifying Bodies
| Please identify your certification program and appropriate acronym. |
FIG Life Care Planning – Certified (FIG LCP-C) |
International Certified Cost for Care Professional (ICCCP) |
International Certified Cost for Care Professional Fellow (ICCCPF) |
Universal Life Care Planning Certification Board (ULCPCB)
Certified Nurse Life Care Planner (CNLCP) |
Universal Life Care Planning Certification Board (ULCPCB)
Certified Health Professional Life Care Planner (CHLCP) |
| Who are the appropriate candidates for your certification program? |
Individuals in medical, healthcare, and rehabilitation fields. |
Practicing rehabilitation professionals with a rehabilitation credential who have been doing or assisting with life care planning but don’t yet have a certification. |
Experienced life care planners with an established credential. |
Licensed registered nurses. |
Licensed health care professionals. |
| How many have you certified and renewed? |
200 certificants with 200 students in the pipeline. |
19 registrants - 8 ICCCP and 11 ICCCPF |
19 registrants - 8 ICCCP and 11 ICCCPF |
|
|
| What are the requirements for your certification? |
A minimum of a bachelor’s degree in the medical, healthcare, or rehabilitation field. An current, active and unrestricted license or certification in a primary practice within a medical, healthcare, or rehabilitation field with a minimum of two years full-time paid employment. Completion of the 120-hour FIG LCP-C course and peer reviewed life care plan. |
ICCCP grandfathering: CVRP credential in good standing or CCRC, CRC, CCM, CVE, CCVE, ICVE or equivalent credential. Confirmation of having completed or co-authored life care plans. Successful completion of a peer-review or redacted life care plan, success passing of the ICCCP exam. Also requires proof of government issues ID and background check.
ICCCP eligibility:
Same requirements as the grandfathering plus completion of college-
approved training including a minimum of 800 mentoring and supervision hours in topics relevant to life care planning. |
Confirmation of possession of a recognized life care planning certification. Three of the following 6: confirmation of testimony defending life care plans, proof of publication of peer-reviewed article in a recognized publication,
experience teaching a life care planning course or through a recognized institution, presenting at a recognized conference, experience peer reviewing for life care plan credentialing, or participation in life care planning exam questions. Completion of the ICCCP exam. Also requires proof of government issues ID and background check. |
Proof of active, valid and unrestricted licensure. Verification of a minimum of 2,000 hours of paid or billable hours of experience in a role that utilizes the nursing process in assessing and determining an individual’s long term care needs and costs within the five years preceding application. Proof of completion of 120 continuing education units related to life care planning or verification of two years of life care planning experience, both within the five years immediately preceding application. |
Proof of current, active and unrestricted licensure in healthcare or a health and human services discipline that allows for the practitioner to perform independent patient/client assessment. Verification of two years/4,000 hours of paid or billable professional healthcare experience with the five years preceding application. Proof of completion of 120 continuing education units related to life care planning or verification of two years of life care planning experience, both within the five years immediately preceding application. |
| What is the fee associated with your certification? |
There is no additional cost for certification, cost is included in price for the LCP-C education program. |
Cost for application is $307.
No cost for applying for CEUs or for renewal. |
Cost for application is $307 plus a one time fee of $209 for the grandfathering of the ICCCPF.
No cost for applying for CEUs or for renewal. |
CNLCP portfolio exam: $495
Recertification by CEUs or portfolio exam: $495
Late recertification: $695
Retesting: $245
*AANLCP members receive a $100 discount on initial certification, recertification, and late recertification. |
Portfolio examination: $395
Portfolio examination retesting: $245
Recertification by CEUs or portfolio exam: $395
Late recertification: $595 |
| Are there pre-approved programs that provide the educational format for your certification program? If so, what are they? |
The certification is available for graduates of the FIG LCP-C education course. |
Not for certification.
There is a pre-approved list of courses for CEUs on the website, as well as options to submit for pre- or post- approval for CEUs from sources not listed. |
Not for certification.
There is a pre-approved list of courses for CEUs on the website, as well as options to submit for pre- or post- approval for CEUs from sources not listed. |
No, but nurses considering CNLCP are encouraged to choose a life care planning program that includes the nurse life care planning process. |
No. |
| Is your certification program accredited and if so by whom? |
No. |
Not currently, but pursuing the ISO 17024 international accreditation through Standards Council of Canada. |
Not currently, but pursuing the ISO 17024 international accreditation through Standards Council of Canada. |
Not yet, but pursuing accreditation through the Accreditation Board of Specialty Nursing Certification (ABSNC). |
Not yet, but pursuing accreditation through the National Commission for Certifying Agencies (NCCA). |
| What are the continuing educational requirements for your certification and how often are they required? |
60 units every five years. |
40 units every two years. At least 6 have to be in Ethics. |
40 units every two years. At least 6 have to be in Ethics. |
60 units every five years with at least 12 units related to life care planning.
60 units every five years with at least 12 units related to life care planning. |
60 units every five years with at least 12 units related to life care planning.
60 units every five years with at least 12 units related to life care planning. |
| What makes your certification special? |
The certification emphasizes competency and not just knowledge. FIG provides support to graduates. Staff members will not oppose fig graduates on cases and are required to conflict out when they see a FIG graduate on the opposing side. |
CVRP does not provide any education. There are policies and procedures with respect to complaints and disciplinary processes and procedures and you can be reported. In order to protect the public background checks are required. |
CVRP does not provide any education. There are policies and procedures with respect to complaints and disciplinary processes and procedures and you can be reported. In order to protect the public background checks are required. |
The certification utilizes a portfolio examination that requires the applicant to show proof of concept of being able to apply each step of the life care planning process to a real world case scenario. This process was developed in conjunction with a professional test incorporation to ensure the process meets the rigors of the national criterion for testing and certification. |
The certification utilizes a portfolio examination that requires the applicant to show proof of concept of being able to apply each step of the life care planning process to a real world case scenario. This process was developed in conjunction with a professional test incorporation to ensure the process meets the rigors of the national criterion for testing and certification. |
| What are your biggest challenges? |
Trying to focus on education and mentorship, certification is only the starting point on life care planning. |
Establishing distinction between college and association being an international organization. |
Establishing distinction between college and association being an international organization. |
Bandwidth issues for those involved, both the board and applicants. And staying afloat in such a small niche industry. |
Bandwidth issues for those involved, both the board and applicants. And staying afloat in such a small niche industry. |
*The International Commission on Health Care Certification (ICHCC) and Certified Physician Life Care Planner (CPLCP) were also invited to participate but declined.
The top strengths of the certifying entities identified by the breakout groups included certification providing greater support and respect/reputation for life care planners and the work they do, having diverse options for certifications, and having a means to test for competency. The top concerns included the number of options available, the lack of uniformity across the available options, and whether there is validity to the certifications in their current state with their varying requirements, standards, processes and lack of oversight/standardization. When asked what the life care planning community needs from their certifying entities to rectify concerns and improve the confidence in the certifications, the top answers included stability and unity across certification programs, greater consistency for receiving and availability of continuing education units, and transparency from the certifying entities.
Professional Associations
| What is your association name? |
American Association of Nurse Life Care Planners (AANLCP+) |
International Association of Rehabilitation Professionals (IARP)/International Academy of Life Care Planners (IALCP) |
| How do you advocate for life care planners? |
Providing education, mentorship and resources, marketing at various forums and platforms, providing core curriculum and standards of practice, community listserve discussion board, volunteer opportunities with committees focused on research, outreach, education, mentorship and publishing. |
Provide educational and mentorship opportunities, host in-person events, have the Journal of Life Care Planning and the Rehabilitation Professional, work with the foundation to promote life care planning research, and have a fellow program for high level practitioners. Provide lots of opportunities for networking and collaboration. |
| How many members do you have that are life care planners? |
100% of members are life care planners. |
IARP has about 1,500 members with upwards of 550 being life care planners. |
| What are your membership demographics? |
AANLCP has members in every state in the contiguous US, the USVI, Canada and Australia.
Estimate ages of members to range from 30 to over 70. |
IARP has a wide variety of backgrounds from various rehabilitation professions and have members across the US and internationally in Canada and Mexico. |
| What are your general education activities annually? |
Annual in person conference, annual virtual conference, and online webinars. |
Yearly in person Symposium in the fall and live webinars and webinar series, as well as co-sponsoring the Summit. |
| Do you have inclusion/exclusion criteria? |
Do not discriminate, everyone is welcome. |
Main requirement is a degree or experience in a field related to the organization. |
| What is the cost of membership? |
Basic: $225 Premier: $475
Retired Professional: $100 Student Basic: $99 Student Premiere: $199 Corporate Basic: $999
Corporate Premiere: $1,999 (corporate memberships provide membership for 5 employees - must be W2 employees) |
Individual Professional: $350 Introductory Membership: $100 Associate: $290
Corporate: $290 - $335 Retired: $125
Student: $25 |
| What are the benefits of membership? |
Basic/Retired Professional: discounted webinar fees, discounted annual conference fees, exclusive discount offers for life care planning resources, access to listserve, voting privileges.
Premiere: free webinar access, annual listing in the Find a Life Care Planner directory, discounted annual conference fees, lifeline mentorship program, internal subcontractor directory, access to life care planning resources and the PMIC medical fees ebook, exclusive discount offers, access to listserve, voting privileges.
*Student and corporate basic and premiere memberships maintain the same benefits as standard basic and premiere. |
Free webinar access, voting privileges, participation in the mentoring program, ability to serve in a leadership role, member discounts to life care planning resources, access to JLCP, and access to the listserve.
In addition to standard membership, student membership includes discounts on IARP events and free membership to state chapters. Corporate membership includes a company listing on the IARP website and a 20% discount on job postings. |
| What opportunities and challenges do the organization have? |
Improving attendance to conferences and webinars, increasing membership engagement, and increasing participation/submission to JNLCP. |
Opportunities include all of the active committees that are working to keep the organization on the forefront of the field and addressing important issues in life care planning. Challenges include how rapidly technology is changing and keeping up with that it, while and addressing how that impacts the field, as well as being a volunteer run organization and making sure we recognize and appreciate all the work being done by the volunteers. |
*The Association of Certified Life Care Planners (A-CLCP) was also invited to participate and declined.
The top strengths of the professional associations identified by the breakout groups included availability of opportunities for networking, mentorship and community support, availability of opportunities for continuing education units, and the diversity of backgrounds that the associations united. The top concerns included the fragmentation and divisiveness that comes from having multiple associations that function independently of each other, the lack of consensus between the associations, and the level of active participation from the associations. When asked what the life care planning community needs from their professional associations to rectify the concerns identified by the participants, the top answers included collaboration between and/or merger of the existing organizations, more opportunities to receive continuing education units, greater availability and access of mentorship opportunities, and up to date information and resources critical to the practice of life care planning.
Part 2: Consensus Statement Review
In the afternoon of day one the large group convened, and a discussion was held regarding the need for analysis and organization of the existing Consensus and Majority Statements. The group agreed to return the following day to embark on reviewing these prior Consensus and Majority Statements.
During day one of the Summit, the attendees were charged with sorting the 96 Consensus and Majority Statements into domains. Consensus was reached among attendees that these would be tentatively titled as follows:
Relevant to the Life Care Planner – Not Found Elsewhere
Relevant to the Life Care Planner – Found Elsewhere
Advisory to Entities
No Longer Applicable.
Sorting was carried out using real time voting via the Mentimeter platform.
Each statement was shown to the group, and they were asked to vote on a category. Each individual was allowed to submit a single vote without the option to go back and change their vote once the group’s data was collected. In keeping with past summit proceedings, majority was set at 75% of votes received; total Summit participant counts were maintained throughout voting and vote counts were tracked in real time by Mentimeter to ensure complete voting and accurate calculation of percent support for each category. If a single category received majority votes, the statement was sorted into the majority domain. Following review of all 96 statements, any statements for which a majority was not reached were revisited with opportunity for open discussion amongst the group, immediately followed by repeat voting. The same threshold for majority was used if a single category received majority votes, then, the statement was sorted into the majority domain.
Upon completion of voting, discussion was held regarding permanent domain titles. Titles were proposed by the participants and by consensus agreed upon by the group. The group arrived at the following nomenclature and accompanying definition for the organization which include:
-
RELEVANT TO THE LIFE CARE PLANNER: Statements originally developed dating back to 2000 by majority and consensus that have been deemed still relevant and applicable to the individual practice of the life care planner.
-
RELEVANT TO THE LIFE CARE PLANNER – PUBLISHED ELSEWHERE: Statements originally developed dating back to 2000 were deemed relevant and applicable to the practicing life care planner that were further reinforced in alternative literature sources.
-
ADVISORY TO LIFE CARE PLANNING EDUCATIONAL PROGRAMS, CERTIFYING BODIES, PROFESSIONAL ASSOCIATIONS AND ORGANIZATIONS: Statements originally developed dating back to 2000 were deemed relevant and applicable; however not directly applicable to the practitioner, but instead agreed to have advisory value to ancillary life care planning entities who oversee the standards of practice, educational programs and certifications, and professional associations and organizations.
-
UNDER FURTHER REVIEW: Statements that are considered relevant to life care planners but in need of review and revision to keep up with current times. These statements still hold relevancy to the life care planner until such time as consensus is reached to modify.
Once the statements were organized into their respective domains, all of the statements within the Under Further Review domain, including all of the statements voted to be no longer applicable and the statements where no majority was reached, were subjected to further review to determine whether they should be accepted in their current state as relevant to the life care planner, modified to become relevant to the life care planner, or archived as historically important but no longer relevant. Statements deemed relevant were added to the Relevant to the Life Care Planner domain, and statements requiring modification remained in the Under Further Review domain. A fifth domain was created for archived statements that would include those voted to delete during the 2025 Summit as well as historically deleted statements. The fifth category was named as follows:
- PREVIOUSLY DELETED, AND NOW HISTORICALLY IRRELEVANT OR NO LONGER VALID: Statements, which were reviewed in 2010, via Delphi methodology in 2018, and in 2025 that were recommended to be archived for historical preservation and removed from the Consensus Statements.
Within these categories the following results reached consensus with a threshold of 75%.
RELEVANT TO THE LIFE CARE PLANNER: 12 Statements
RELEVANT TO THE LIFE CARE PLANNER – ALSO PUBLISHED ELSEWHERE: 41 Statements
ADVISORY TO LIFE CARE PLANNING EDUCATIONAL PROGRAMS, CERTIFYING BODIES, PROFESSIONAL ASSOCIATIONS AND ORGANIZATIONS: 15 Statements
UNDER FURTHER REVIEW: 15 Statements
PREVIOUSLY DELETED, AND NOW HISTORICALLY IRRELEVANT OR NO LONGER VALID: 13 Statements (plus 3 previously deleted statements)
A full updated reprint of the Consensus and Majority Statements since 2000 has been updated at the 2025 Life Care Planning Summit is available and included in a document published in this issue.
Discussion
As life care planning evolved, it was necessary to aid in its construction. Summits aided in that process and continue today. The results of the 2025 Summit were a continuation of the advances made within the specialty practice and acknowledgement of the diversity of profession, geography and practice type of the practitioners, and the inclusion of all. The process of reviewing, updating, guiding, and developing best practice was and continues to be important work completed by life care planners for life care planners, about life care planning. This Summit was no different. The attendees agreed that there is work to be done and the outcome of this Summit should serve as a charge for educational programs, certifications, professional life care planning associations and organizations to review this proceeding and consider the recommendations for future action.
Conclusion
As history has shown, evolution occurs. When the original 2000 Summit occurred, it was the early in the evolution of the specialty practice of life care planning. Twenty-five years later, the growth within this practice and dedication of the practitioners has created a long-standing guidance which requires monitoring and evaluation to remain current. However, it is essential to be mindful of the past and strive for a better future at all levels including those entities which support, develop and encourage life care planners in their daily work.
Attendees
| Tracy Albee |
Heidi Fawber |
Andrea Nebel |
| Michele Albers |
Brook Feerick |
Zarahi Nunez |
| Holly Allman |
Ellen Fernandez |
Erin O'Connell |
| Lisa Anderson |
Michelle Fleury |
Dana Penilton |
| Rebecca Bailey |
Shelene Giles |
Elizabeth Peralta |
| Kimberly Beladi |
Rachel Gooding |
Edmond Provder |
| Debbie Berens |
Janet Gowing |
Jason Purinton |
| Harold Bialsky |
Susan Guth |
Paul Ramos |
| Stephanie Birely |
Kelly Harvey |
Scott Ranney |
| Alana Bomberger |
Patty Hedrick |
Rhonda Renteria |
| Nancy Bond |
Jocelyn Holt |
Sherry Ribble |
| Madysen Bowen |
Jennifer Holt |
Jan Roughan |
| Brandy Bradley |
Cloie Johnson |
Carolina Salazar |
| Erika Browning |
Elizabeth Kattman |
Julie Sawyer-Little |
| Susan Burke |
Shelly Kinney |
Linda Schwieger |
| Todd Capielano |
Trudy Koslow |
Scott Sevart |
| Darlene Carruthers |
Sarah Larsen |
Kate Smith |
| Hantac Chang |
Ashley Lastrapes |
Ron Smolarski |
| Tony Choppa |
Sherry Latham |
Stella Spencer |
| Nick Choppa |
Amy Mackenzie |
Victoria Spruance |
| Warren Comeau |
Sarah Malloy |
Gil Spruance |
| Dawn Cook |
Sylvia Ann Maniha |
Rachel Stone |
| Aubrey Corwin |
Debbe Marcinko |
Amy Sutton |
| Jenn Craigmyle |
Michael Martinez |
Miranda Van Horn |
| Becky Czarnik |
Sonia Masuga |
Charlotte Warmington |
| Heather Dahl |
Chris McDermott |
Deborah Watkins |
| Maria Rizza Dalisay |
Holly McLendon |
Lora White |
| Brian Daly |
Nicole McManus |
Caroline Williams |
| Kelly Dawson |
Jacqueline Mendez |
Susan Wirt |
| Christina Dillahunt-Aspillaga |
Teresa Millsap |
Aaron Wolfson |
| Emily Dillard |
Courtney Mitchell |
Laura Woodard |
| Katherine Dunlap |
Lindsay Moore |
Vanessa Young |
| Stephanie Engler |
Michelle Moore |
David Zak |
| Dawn Espinoza |
Tricia Morrison |
Elizabeth Zaras |
Letters of Support and Endorsement from Leaders in the Field
The following letters were submitted after the 2025 Life Care Planning Summit by attendees. We are grateful for their continued support.
From Debra E. Berens, Ph.D., CRC, CCM, CLCP, Secretary for Foundation for Life Care Planning and Rehabilitation Research (FLCPRR):
On behalf of the Foundation for Life Care Planning and Rehabilitation Research (FLCPRR), we would like to thank the IALCP and the 2025 Summit committee for your tireless efforts to plan and host the 2025 Life Care Planning Summit. The Committee’s energy and enthusiasm during the Summit was obvious and contributed to keeping the participants engaged throughout the 2-day meeting. The Educational session on day 1 was helpful for attendees to learn about life care planning related programs and organizations; thank you for allowing the FLCPRR to participate as a featured organization in that portion of the Summit. I would also like to recognize the hard work of the Summit committee in being responsive to the needs of life care planners and related life care planning professionals. The shared purpose and shared experience of the participants to review the Consensus Statements is a challenging task and your committee presented the information in a way that fostered connection, community, and greater understanding among the participants. Even more impactful is assuring that the outcome produces a cohesive and consistent Consensus Statement document that serves as a useful tool to guide life care planners to succeed into the future. Once again, the FLCPRR thanks the IALCP and the 2025 LCP Summit Committee members and supports their efforts for enhancing the Consensus Statements. We look forward to the published proceedings and the updated Consensus Statement document.
From Nick Choppa, M.A., CRC, CCM, CDMS (Past Chair, IALCP):
The 2025 IALCP Summit was an excellent opportunity to collaborate with the broad and trans-disciplinary field involved in the specialty practice of Life Care Planning. Bringing over 100 members together to review the Consensus and Majority statements, and actually reach consensus over the course of two days was a phenomenal process. The organizers were highly prepared and the results show. All attendees were engaged in a vigorous debate and discussion about this specialty practice, and continue to pave the way as leaders in the field for how this work is and should be performed.
From Warren Comeau, CCRC, (F)CARP, CVRP(F), ICCCP(F), Life Care Planner, Atlantic Canada:
Summit 2025, which took place in Minneapolis last month, was my first opportunity to participate in what I understand have been gatherings of life care planners in similar forums over the past 25 years. Our goal was to consider the Consensus and Majority Statements which have guided the direction of our subspecialty field for over two decades. Keeping over 100 life care planners on task over two days, professionals from varying educational and experiential backgrounds, and arriving at consensus on what to do with 96 Consensus and Majority Statements, is no easy task. Well-earned kudos are definitely deserving to our facilitators, Cloie Johnson, and Brook Feerick and Amy MacKenzie, for their skill and determination in encouraging continual diverse commentary and input throughout the process. There was also an opportunity to hear previously recorded video interviews from a number of life care planning credentialing and education bodies, and a chance to discuss this information in break- out groups. The masterful coordination in the use of voting software made it possible for everyone’s vote to be seamlessly tallied at each juncture, for each of the 96 statements (well done, Dr Caroline Williams!). The University of Minnesota’s McNamara Alumni Centre (well done, Paul Ramos) is a beautiful and impressive venue. The friendly staff of The Beacon at the Graduate Hotel provided an atmosphere of good cheer for our after-session gatherings and refreshment. Well done everyone!
From Becky Czarnik, MS, RN, CNLCP, CMSP-Fellow:
I had the honor of being part of the working group for the consensus statements and subsequently attending the 2025 Summit to engage in the final voting process. This huge undertaking involved considering multiple perspectives. At the Summit, we were organized into breakout groups that included representatives from various professional backgrounds relevant to our roles as Life Care Planners. Each step of the process involved thoughtful (and occasionally passionate) discussions on how each consensus statement would impact our individual practice and professional role. I was impressed by the civil discourse that occurred both within the small groups and the larger assembly. Ultimately, we discovered that, despite our diverse professional backgrounds, we share more commonalities than previously assumed. The entire Summit process was respectful, engaging, and provided valuable experience to the Life Care Planner community.
From Heidi Fawber, M.Ed., LPC, CRC, CCM, CLCP, FIALCP:
I would like to comment on the recent IALCP Summit held in Minneapolis MN on May 16 and 17, 2025. It is remarkable to reflect on my participation in nearly every Summit since 2000. This year’s event instilled in me a deep sense of pride in being part of the life care planning community. Over a year ago, numerous life care planners began preparations for the 2025 Summit, under the leadership of Brook Feerick and Dr. Amy McKenzie (co-chairs) and Cloie Johnson and Dr. Caroline Williams. The dedication and work ethic exhibited by this group of professionals are unparalleled.
Building on the Summit’s history, the 2025 Summit Workgroup Committee devised a framework for the revision of Consensus Statements, ensuring collective feedback and support from the life care planning community. After extensive reviews of the Consensus Statements by the 2025 Summit Workgroup, a framework of categorization of the Statements was proposed for Summit participants’ review and feedback. Attendees engaged in small group discussions on various topics relevant to life care planners, including Education & Training Programs, Professional Organizations, and Certifications, leading to highly interactive dialogues. Subsequently, a full-group meeting was held to discuss the optimal approach to Consensus Statement categorization and revisions, with real-time voting facilitated through Mentimeter. Participants diligently explored diverse opinions regarding Consensus Statements and their perspectives on contemporary life care planning practices. These insightful discussions and varied viewpoints made me optimistic about the future of life care planning Summits with the collective goal of embracing the history and value of Consensus Statements and working towards revisions that are consistent with our professional standards and ethics. I look forward to continuing committee work with the dedicated life care planners whom I had the pleasure of collaborating with during the 2025 Summit.
Shelly Kinney, MSN, RN, CNLCP, CCM:
As a first-time attendee at the 2025 Life Care Planning Summit, I found the experience overwhelmingly positive. The sense of camaraderie among life care planners from diverse backgrounds was truly inspiring. Participants demonstrated a strong collective commitment to achieving consensus on key questions and statements. The Summit’s leadership demonstrated deliberate efforts to ensure all voices were heard and that each attendee’s perspective was respected and valued. While there remains important work to be done to ensure the Summit fully reflects the diversity of the life care planning community, it was clear this priority is well recognized and that concrete steps are being taken to advance progress in this area. I look forward to contributing to the ongoing efforts between Summits and to participating in future gatherings.
From Trudy R. Koslow, M.Ed., CRC, CCM, CLCP, ABVE/D:
During the early years of the development of life care planning as a specialized practice area, practitioners in the field began developing Consensus and Majority Statements to assist with the development of the field including standardization and methodology concerns. As the practice evolved, Standards of Practice in life care planning and Ethical Standards in various occupations were developed. To review all the Consensus and Majority Statements that were developed over the years, Summit attendees were asked to consider the necessity of all the current statements in light of current life care planning practice. For context purposes, the history of the Consensus and Majority Statements, the current life care planning training programs, current certifications, and professional organizations life care planning were provided by the Summit organizers. The attendees were then asked to consider whether the Consensus and Majority Statements remained relevant. The voting was done via an app, which registered responses in real time. If questions remained, further discussion was done.
By this method consensus was achieved on several of the statements. Although further work remains to be completed, the Summit provided all life care planners who attended with a frame of reference for the Consensus and Majority Statements, and where we go from here.
From Debbe Marcinko RN BSN MA CRRN CCM CRC CLCP CNLCP ICCCP(F):
I had the privilege of attending the 2025 Life Care Planning Summit: Aligning for Consensus – Past Foundations to Future Needs. As a participant I am pleased to endorse the results and proceedings of this Summit. The Life Care Planning Summit continues to be the unified voice of all life care planners: seasoned practitioners and those new to the practice, from a variety of backgrounds. As with prior Summits, this Summit was organized and a positive collaborative event. The Delphi method was productive in gathering the group’s expertise and consensus in organizing the consensus statements. Discussions were lively and educational. Areas for future dialogue were identified. Consensus statement’s role, compiled since 2000, have created a foundational document for life care plans and have been affirmed by court decisions. Thank you to the coordinators and facilitators for their effort and commitment to the Life Care Planning Summit’s purpose and process. I encourage all life care planners by their participation to be a voice in the future of life care planning.
From Tricia Morrison, PhD, OT Reg., (ON), CLCP, ICCCP(F), FIALCP:
It was my genuine pleasure to serve as a member of the working group tasked with examining the consensus and majority statements in anticipation of Summit 2025. This analysis demanded a deeper immersion into the statements than I had previously undertaken, as well as careful consideration of the underlying intent, function, and enduring significance of each statement. After a year of work, we approached Summit with a sense of positive momentum, focused on organizing our guiding principles into a cohesive, contemporary framework that also respects our historical foundations. As anticipated, the discussions and processes leading up to and during Summit were messy and at times contentious—and that’s exactly as it should be! Critical decisions are being made and should be examined from multiple viewpoints. The leaders provided clear instructions and guidelines, encouraging participants to collaboratively chart the path forward. Through dedicated and sustained effort among all involved, we made meaningful progress and produced a product that is both valuable and actionable. While there is still work to be done—such as refining the wording of certain statements—we can all take pride in having contributed to our community’s collective advancement in this important endeavor.
From Paul Ramos, PT, GCS, CLCP, FIALCP, ATP, CEAC PMR Med Legal:
I would like to express my strong support for the 2025 Life Care Planning Summit Proceedings held in May in Minneapolis, Minnesota. The summit was a testament to the dedication, professionalism, and collaborative spirit of all participants who contributed their time, expertise, and insight. The process was marked by exceptional teamwork and mutual respect, fostering positive group dynamics that led to meaningful discussions and a well-earned consensus on many critical issues facing the field. The hard work invested by the organizing committee and attendees alike resulted in a meaningful reshaping of our consensus and majority statements and laid a foundation for the continued advancement of life care planning. This collective achievement underscores the summit’s importance in shaping the future of our profession.
From Gil Spruance MS, CRC, CVE, CCM, CLCP, MSCC:
I had a chance to attend the two-day Summit in Minneapolis. I previously attended a number of Summits, including 2017 in Denver and 2022 in Ft Worth. The 2017 Summit was primarily an in-depth review of our consensus statements. Day two in Minneapolis was also a review of consensus statements. It was very well run and orchestrated, including a volume of work by our peers pre-Summit, and a home-work assignment (questionnaire) prior to attending. 100+ Life Care Planners from across the country and Canada, with varying amounts of experience and professional backgrounds, all with exceptional insight and opinions! It was a task to get this group through the objectives of categorizing the consensus statements and determining which ones needed further work. Reviewing and updating consensus statements are critical to our profession and will be a never-ending process! Walking 100+ exceptional Life Care Planners through the process is a daunting task! And the Minnesota experience was absolutely a work of art! Well done!! I look forward to the next Summit!
From Elizabeth Zaras, MSN, RN, FNP-C, CLCP (Current Chair, IALCP):
Being part of the IARP/IALCP Summit felt a little like professional spring cleaning—sorting through what still fits, what needs mending, and what it’s time to let go of. It was an invaluable experience that demonstrated the strength of collaborative, consensus-driven work among experienced professionals. The structured review and thoughtful reorganization of the consensus statements reflected both the maturity of our field and the importance of staying responsive to its evolving demands. The process and our fearless Summit leaders were transparent, inclusive, and productive, encouraging dynamic discussion while steadily moving toward shared understanding and agreement. The end result is a sharper, more relevant set of statements that reflects where our field is now and where it’s heading. I truly appreciated the structure of the Summit and the respectful, dynamic way consensus was built. It’s a model I will gladly follow again.