
Historically, life care planners have met at summit meetings to develop consensus on emerging issues and best practices for more than two decades (Rutherford-Owen et al., 2024). Outcomes from these summits were published to become the Consensus and Majority Statements (Johnson et al., 2018), which are agreed-upon best practices used by life care planners and updated regularly. In the past, the nominal group technique and the Delphi technique assisted with consensus development during the summit meetings (Rutherford-Owen et al., 2024). At the 2022 Summit, Top Hat, an interactive technology platform, was used to collect participants’ responses as a supplemental tool along with the use of a skilled facilitator and transcriber for focus groups. Peer-reviewed studies have shown that the Top Hat platform provides raw data that can be exported for later qualitative data analysis (Cooper, 2024; Costa et al., 2022; Feicht et al., 2020; Wismer et al., 2021), and focus groups are established data collection mechanisms for qualitative methodology (Luke & Goodrich, 2019).
Summit participants were informed that Summit results would be presented in a peer-reviewed publication with attendee recognition (Johnson et al., 2023). The organizing committee analyzed the survey data collected at the 2022 Summit, consistent with the aforementioned techniques used in prior summits, where findings were collected and published. This chapter presents the methods and findings of this qualitative data analysis using the 2022 Summit Top Hat data and discusses how the results can be beneficial to the life care planning practice as well as potential study limitations, and recommendations for future research.
Purpose of This Study
The purpose of this study was to perform a qualitative data analysis using the 2022 Summit Top Hat data. During the summit, participants responded to focus group questions using the Top Hat platform, then “liked” the responses. Participants were instructed that a “like” indicated a comment they wanted to discuss further. The data from both focus group sessions were saved on Top Hat for later qualitative analysis. The first focus group session involved questions regarding costing techniques, along with strengths and challenges associated with each technique. The second session addressed the techniques used when preparing and receiving questions during testimony. The purpose of the focus groups was to allow participants to openly discuss costing techniques used in a life care plan (Johnson et al., 2023). Thematic analysis was chosen to identify themes from Top Hat data saved from the focus group questions and data that represented the “liked” or considered most important topics by the participants. The themes would help better understand the costing techniques that life care planners were using as well as the information when preparing and testifying regarding their use, and the strengths and challenges that influenced those choices. During a verbal discussion of the most frequent “liked” responses, a transcriber saved responses for later analysis. (See Chapter 6 for qualitative analysis of the transcribed responses.)
Methods
2022 Summit Participants
The IALCP Summit, held on May 13-14, 2022, was attended by 161 life care planners at the Dallas-Fort Worth Airport Hyatt Hotel. More than 39% of Summit attendees had been completing life care plans for over 20 years, and 64% for over 10 years (Johnson et al., 2023). The primary certification or professional discipline of participants was certified life care planner (CLCP®; 64%) certified nurse life care planner (CNLCP; 22%), certified rehabilitation counselor (CRC; 21%), and certified case manager (CCM; 18%) (Johnson et al., 2023).
Study Procedure
Prior to the summit, Jamie Pomeranz, PhD, CRC, CLCP, and Nami Yu, PhD, CRC, uploaded costing-technique questions, created by the summit committee, into the Top Hat platform, and attendees were provided access to download the Top Hat app. During the 2022 Summit, Dr. Pomeranz and Dr. Yu introduced Top Hat technology, an interactive online platform, and requested that attendees use the Top Hat app to provide responses during the focus group sessions using their personal electronic devices (laptop, tablet, phone). Attendees also received a one-hour training session on using the Top Hat platform.
Following the training session, during Focus Group Session 1, Dr. Pomeranz presented questions one at a time, allowing 3 minutes for participants to review and comment anonymously in the Top Hat online platform. Comments were recorded in real time and visible on participants’ devices. Next, participants were instructed to “like” the comments from focus group questions that they wanted to discuss further or respond with additional comments, allowing 2 minutes for each Session 1 focus group question. Participants responded anonymously and could “like” responses they agreed with, helping the facilitator to identify the most popular topics for further discussion. Participant response rates varied from question to question and are reflected in the analysis for each question. Then, the facilitator ranked the responses that participants “liked” the most frequently; 10 minutes per question were allotted for participants to discuss the top-ranked responses verbally with the use of a microphone. (This data is analyzed in Chapter 6.) Participants were asked to use the same procedure on Top Hat in Session 2 focus group questions the following day as they had in Session 1 using identical procedures.
At the 2022 Summit, participants indicated the need to develop a costing framework to help guide the life care plan costing process, and Dana Penilton and Laura Woodard were assigned as co-chairs by the Summit planning committee to lead this project. A call for volunteers for this project was sent to International Academy of Life Care Planners (a section of the International Association of Rehabilitation Professionals), American Association of Nurse Life Care Planners (AANLCP), and American Association of Physician Life Care Planners (AAPLCP) on July 18, 2022, and closed on October 7, 2022. All participated except AAPLCP. Thirty-five life care planners were chosen to participate in a working group, and 21 people were chosen to be on the advisory committee. From the working group, individuals further volunteered to participate in various subcommittees such as the Top Hat subcommittee (Johnson et al., 2023). The Top Hat subcommittee of six members met regularly from February 2023 until completion of the chapter.
The Top Hat Subcommittee was tasked with reviewing the qualitative data electronically logged during both summit focus group sessions. A quorum of three was required for meetings to review the data and decisions were made by consensus. A spreadsheet was used to analyze the responses, which consisted of initial comments, number of likes and any secondary comments. A tab in the spreadsheet was created for each question. There was a total of 17 questions addressed by summit participants and 17 corresponding spreadsheet tabs. The participants’ information was de-identified before the data reached the committee for analysis.
In the first phase of the analysis, common themes were identified based on the comments provided by participants. Each comment was entered into a row on the spreadsheet, and the comments were reviewed to identify common themes. Columns were created for each theme and the comments in each row were categorized by theme. The themes identified differed for each question to best reflect participant comments. There was also a category of outliers for responses that did not align with the question.
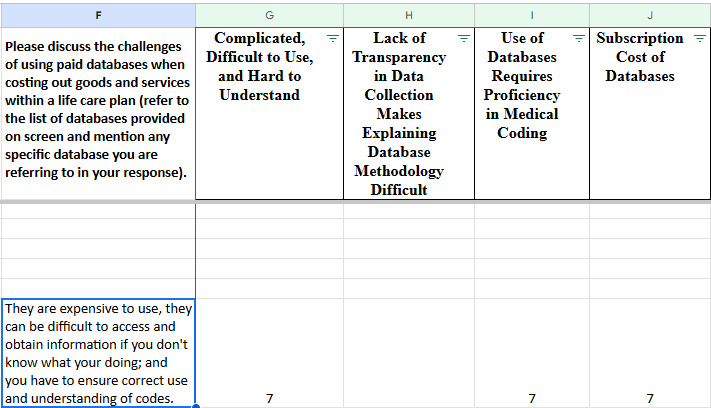
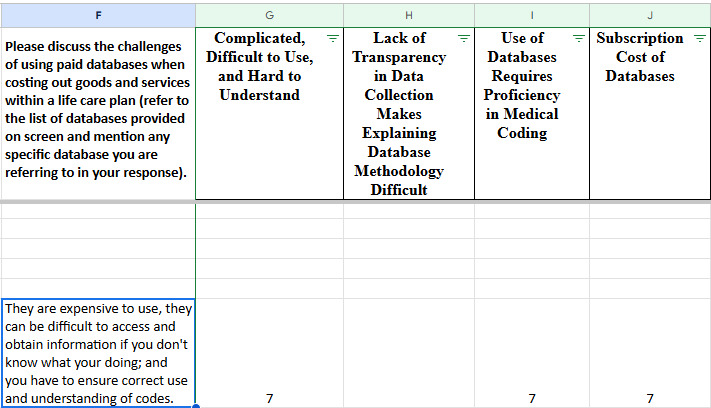
For each row, a number was placed in the column for the theme that the comment fell under, reflecting the sum of the initial comment, the number of likes, and the number of secondary comments. In this way, the total number of responses to each question was captured. Some comments reflected more than one theme and thus were broken apart and categorized under each appropriate theme. An example of this is found in the question asking participants to discuss the challenges of using paid databases. One participant responded that, “They are expensive to use, they can be difficult to access and obtain information if you don’t know what you’re doing; and you have to ensure correct use and understanding of codes.” Reviewers determined that this comment fell under three different themes: Complicated, Difficult to Use, and Hard to Understand; Use of Databases Requires Proficiency in Medical Coding; and Subscription Cost of Databases. There were six likes to this comment plus the comment itself, and therefore, a value of seven was placed under the three different themes, as shown below. This resulted in there being more responses than respondents to acknowledge both the comment and the subsequent “likes.”
Following theme identification, the comments for each theme were copied and pasted into the ChatGPT Artificial Intelligence (AI) tool, using the prompt “what theme would the following comments fall under?” The subcommittee reviewed the original wording compared to themes generated by AI and agreed by consensus to use the original wording, modify the original wording, use the AI-suggested wording, or modify the AI-suggested wording to ensure that the themes accurately reflected the participants’ comments and terminology used in the practice of life care planning.
To quantify the qualitative data, the response count for each theme was divided by the total number of responses per question to yield the percentage of responses that pertained to each theme; this is reflected in a bar graph for each question.
Results
The Top Hat Subcommittee received the de-identified qualitative data saved in the Top Hat platform from the 2022 Summit for analysis. A tally of comments plus likes was placed on the spreadsheet for each theme found in focus group questions. The decision to identify themes was conducted through a collaborative effort from the subcommittee member quorum. When each statement was reviewed, consensus was reached about whether the statement was related to the question and placed within the appropriate theme. The following tables represent the themes identified during qualitative analysis and each theme is followed by examples of comments representing the theme. Each comment is a direct quote of the Top Hat respondent without grammatical corrections.
Within each question there were responses that did not answer the question asked and these were categorized as “Response Does Not Align with Question.” One example of this is the question “Please discuss the use of the 80th percentile as opposed to 75th, 50th or 25th percentile as your industry standard when costing” and the response “GO STARS!” Some responses were not clear enough to discern the writer’s intent and the subcommittee members decided against making guesses as to their meaning. Others were relevant to the subject but not to life care planning specifically. The comment “Can go back in time for bill reviews” in response to the question "Please discuss the strengths of using paid databases when costing out goods and services within a life care plan (refer to the list of databases provided on screen and mention any specific database you are referring to in your response) is an example. The question was specific to life care plan costing, not bill reviews. Participants sometimes commented with a challenge when the question asked for a strength or vice versa. The respondents had the opportunity to voice their comments for the strength or challenge during other questions.
There were also times where discussions ensued between participants within the comments. For example, the question about information prepared regarding medical billing before testifying prompted the following responses [Sic]: “This is sort of out of contesct, but the attorney gets his 33-40% along with the costs, so the lcp is already underfunded from the get-go. why go with such an minimal approach to medical care in the future?,” “Same with expert fees re: Vaccine Compensation Fund,” “Attorneys do not always get paid from the settlement (e.g,., Vaccine Compensation Fund),” and “expert fees are also a part of those fees.” At times, these comments seemed to identify areas where future research or education may be beneficial.
Telephone Calls
Question 1: “Please discuss the strengths of using telephone calls when costing out goods and services within a life care plan.”
Themes Identified & Representative Examples
Fills Data Gaps When No Other Source Exists
-
“Useful for support care (HHA, CNA, RN etc.) and therapy.”
-
“Utilize for HHA, Nursing Facilities etc… as data base not available”
-
“There is niche information that databases cannot gather that is only obtainable from directly communicating with providers.”
Data Integrity (Verifiable, Valid, Reliable, & Accurate)
-
“Good way to compare the database information that you have”
-
“Valid and reliable”
-
“Help support which database percentile is representative for that service”
-
Enables Life Care Planner to Obtain Detailed Service-Specific Costs
-
“Able to have a conversation and in that conversation, some nuance may arise that can be discussed.”
-
“You can call a billing / coding person for a surgeon, for example, to obtain the exact cpt codes for a complex surgery.”
-
“…the opportunity allows for a discussion with the provider of what other services should be included validation of any other professionals or products to be included to support the service…”
Enables Life Care Planner to Obtain Detailed Service Specific Costs
-
“A phone call allows for clarifying questions to be asked and for additional information to be accessed that may not be included on an internet website, database, etc.”
-
“You can call a billing / coding person for a surgeon, for example, to obtain the exact cpt codes for a complex surgery.”
-
“Able to get charges from treating providers that are current and reflect level of complexity of care required by individual.”
-
“Good for obtaining local costs. Can also ask questions about the particular service and if that provider can actually provide them.”
-
“Current data, verifiable with the source details, clarifications as to U/C versus inflated rate to be submitted to insurance.”
-
“Direct vendor survey, for prices not on data bases, eg a MDT pain program, drivers rehab, equipment - with geographical location.”
-
“Attendant care is subject to rather rapid changes geographically and must be tailored to the person’s specific needs. It is an area that lends itself to phone surveys.”
Localized & Geographically Specific Cost Data
-
“Helpful when services are in a rural area with very limited number of providers/specialists and GEO zip includes a significantly large area”
-
“Obtains geographic costing for that particular LCP.”
-
“Able to get information otherwise unavailable for local area”
Current & Up-to-Date Costs
-
“Current”
-
“Up to date”
-
“The up-to-date pricing is also very useful.”
Question 2: “Please discuss the challenges of using telephone calls when costing out goods and services within a life care plan.”
Themes Identified & Representative Examples
Time Consuming
-
“Getting to the right person, time wasted on hold”
-
“Getting information when you are on a deadline in a timely manner”
-
“Time-consuming”
Accuracy, Methodology and/or Reliability Concerns
-
“Inconsistent responses, based on who you speak with/when.limited reproducibility.”
-
“The person on the line may not provide accurate information”
-
“Responses are highly dependent on the way the question is asked. Billed vs. Non-Discounted vs. Charges”
-
“Reliability issues. Not a valid or statistical representative sample of universe of doctors performing the service.”
Non-Responsive/Difficult to Connect (including access to the correct person)
-
“Getting people to answer your call or answer your message and get back with you.”
-
“Providers unwilling to speak to LCPrs.”
-
“Staff have no idea what you want and are fearful of why you want it. NO HEALTHCARE COST TRANSPARENCY”
Hearsay
-
“Sanchez/Case specific hearsay.”
-
“In some states, phone calls are hearsay so we have to provide additional foundation for opinions.”
-
“Hearsay issue.”
Persistent Marketing from the Entity
- “After you get a quote, the agency or facility calls daily hoping you are going to place somebody right away.”
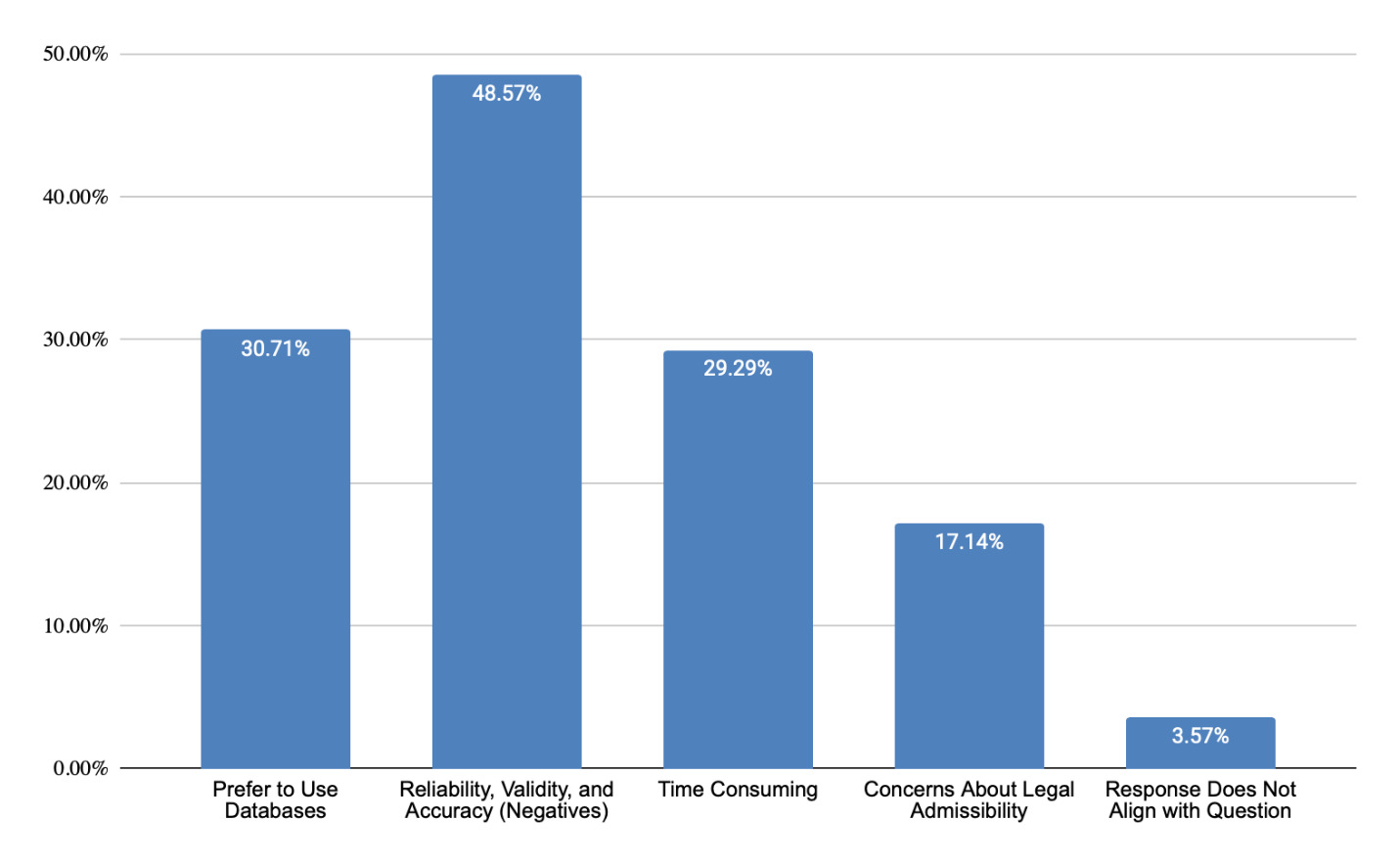
Question 3: “If you do not utilize telephone calls as a technique, please explain why.”
Themes Identified & Representative Examples
Prefer to Use Databases
-
“Rarely used because i understand the cpt codes, DRG groups and the data repositories are statistically reliable - the ICD codes in the file support the services that are being recommended in the LCP”
-
“Lack of time, too hard to get people on the phone or to call you back, prefer databases; only use it when I have no other options.”
-
“I only use them for items that do not have a CPT code.”
-
“PFR has 50, 75, and 90 to show a range of multiple inputs in a geographic area. This can be argued that it is more robust and lessens the outliers. Additionally, it is easily verifiable if opposing expert/counsel wishes to subscribe to the source.”
Reliability, Validity, and Accuracy (Negatives)
-
"Information may not be reliable/accurate. "
-
"Too small a data pool to be reliable "
-
“Not representative of how the medical/healthcare/rehabilitation providers identify their costs outside of the LCP industry.”
-
“Inconsistent results; validity; not statistically supported”
-
“Because the information obtained is extremely biased and unreliable. You are unable to talk with someone who is actually knowledgeable and able to provide the specific information you need. Unreliable therefore there are much better ways to obtain the information that is not only reproduceable but able to be validated and not questioned in the LCP.”
Time Consuming
-
“I don’t have time to sit on a phone and wait for responses to call me back.”
-
“Too time consuming.”
Concerns About Legal Admissibility
-
“Heresay.”
-
“In CA it’s hearsay.”
Paid Databases;
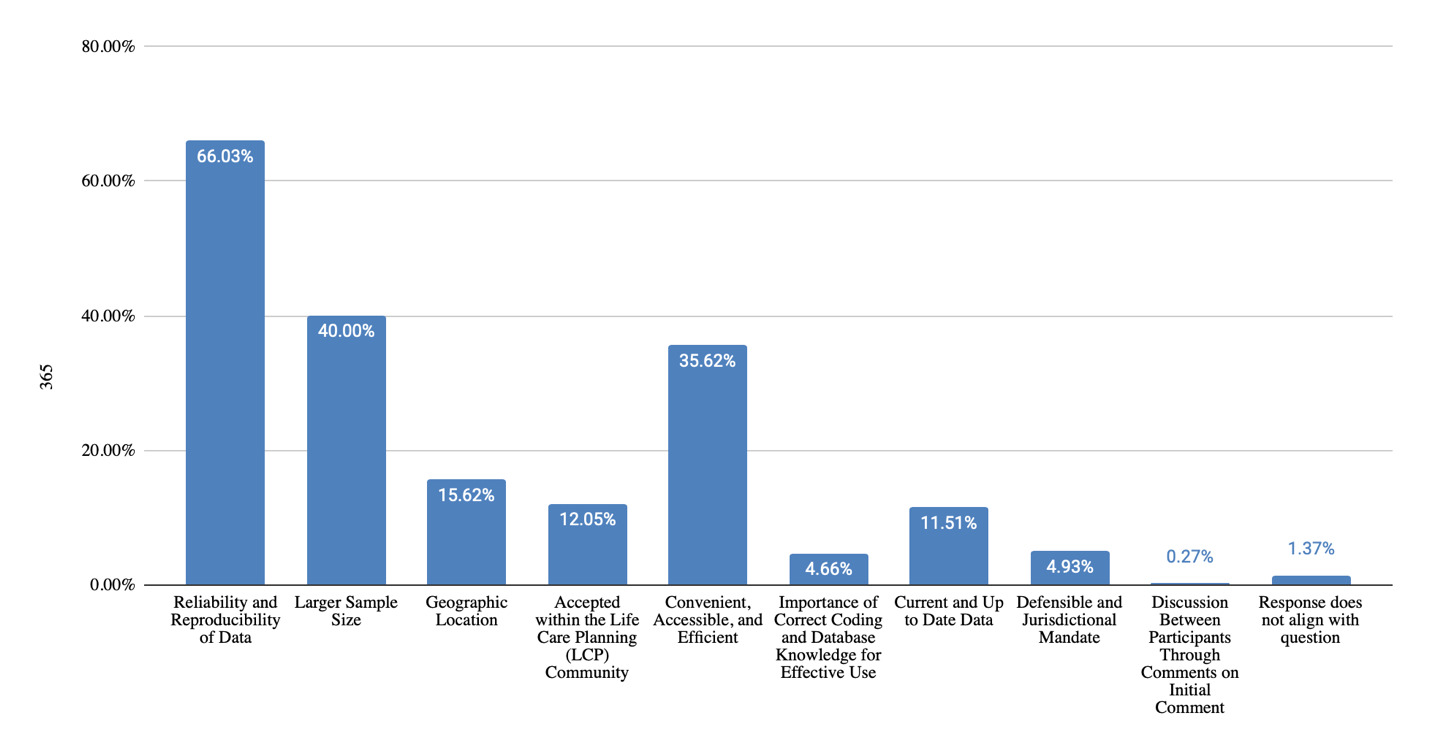
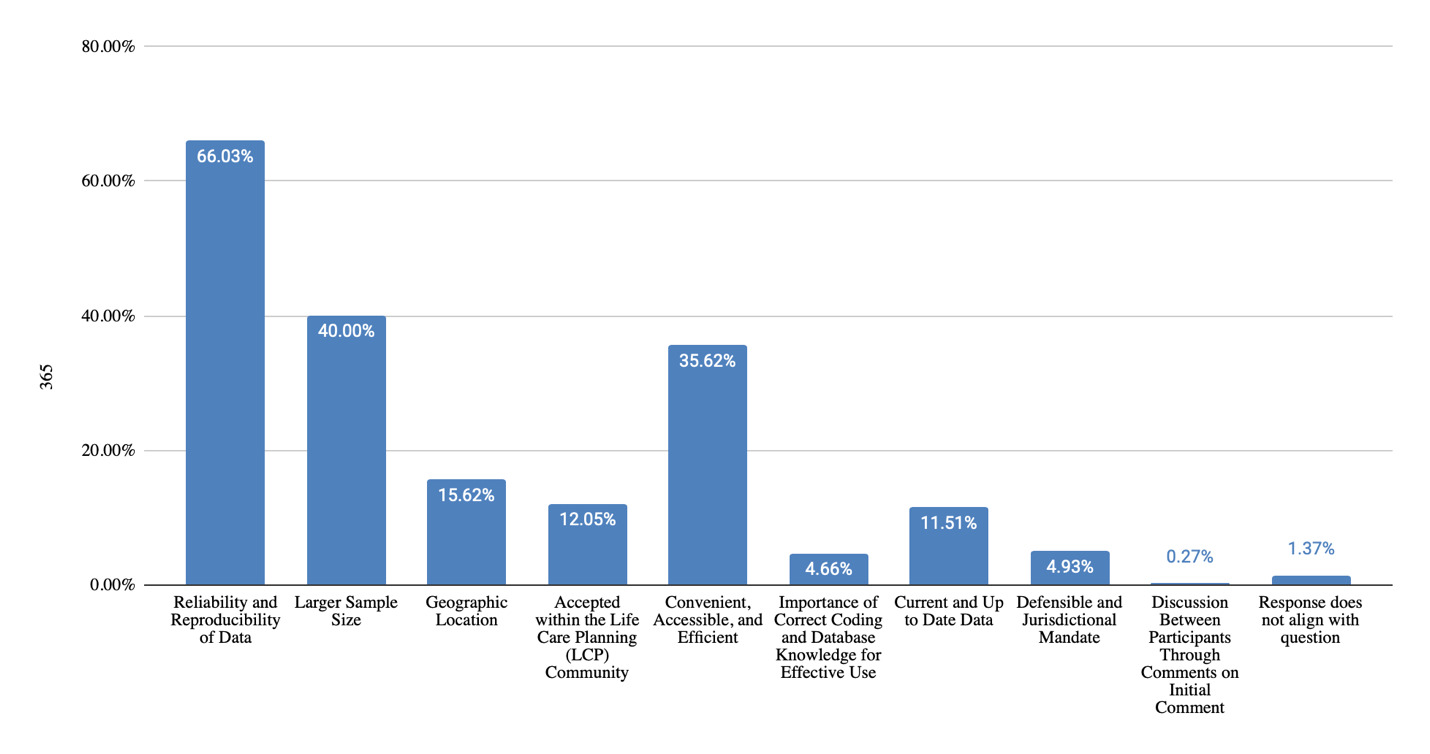
Question 1: “Please discuss the strengths of using paid databases when costing out goods and services within a life care plan (refer to the list of databases provided on screen and mention any specific database you are referring to in your response).”
Themes Identified & Representative Examples
Reliability and Reproducibility of Data
-
“Extremely verifiable and defendable.”
-
“Reliable and can refer to them when you cannot get the information via the phone.”
-
“Credibility and reliability-defensible”
-
“They are reproducible and able to be replicated during deposition or trial. You can go back into the database and enter the date the LCP was completed to verify and replicate the cost. Most beneficial method to determine a valid price that is easy to defend when needed.”
-
“Reliable. Reproducible. Additionally, they are not available to the general public and boost the expert’s value to the case.”
Larger Sample Size
-
“Paid databases offer millions/billions of datapoints to back up their information.”
-
“Based upon a statistically significant data pool”
-
“1,000 - 1,000,000s of providers input to these databases.”
-
“There are comprised of millions plus of charges”
Geographic Location
-
“It uses multiple costs from providers in the area not just one”
-
“Nationwide information that can be dialed down to geographic area”
-
“I feel that the values received are a good representation of the area.”
-
“They allow for geographically appropriate costs.”
Accepted Within the Life Care Planning (LCP) Community
-
“Being used by many LC planners.”
-
“Very common source at this point in time for the profession”
-
“The databases which are considered credible in the industry are a great way to use time management and obtain accurate costs.”
-
“They have become industry standard and not just for purpose of life care planning.”
Convenience, Accessibility, and Time Efficiency
-
“More convenient than making calls.”
-
“For facility fees and surgery costs it would be super difficult to do without databases”
-
“Wide range of costs available in one place. some have codes and costs which saves time”
-
“Fast and easy”
Importance of Correct Coding and Database Knowledge for Effective Use
-
“If you understand the coding systems a great resource”
-
“The data bases (Find A Code, Context 4 Healthcare and Fairhealth are relatively easy to use to obtain costs when you have appropriate CPT codes.”
-
“Accurate, reproducible, reliable, efficient (if educated on the databases and coding).”
Current and Up to Date Data
-
“They are quality controlled, current, and easy to use.”
-
“Updated routinely so you know you are getting the most recent and reliable information”
-
“Generally up to date”
-
“Researchers have already gathered a credible sample and update these costs yearly”
-
“Fair health collects billions of charges in geozips that is updated every 6 months to give you the most updated information”
Defensible and Jurisdictional Mandate
-
“At least one database, FH, provides support if the data is challenged In certain states, they actually refer to specific databases (FH, Wasserman PFR) in their regulations - solid to use in the courts”
-
“Support for challenges”
-
“Most ability to be admitted under Sanchez ruling in California”
-
“Credibility and reliability-defensible”
Discussion Between Participants Through Comments on Initial Comment
-
Initial Comment: “Fair health collects billions of charges in geozips that is updated every 6 months to give you the most updated information, This can then be coupled with phone calls to determine it’s reliability.”
- Response: “Other databases are web-based and updated much more frequently, why would you want to use a price that is at least 6 months old at the time you are doing the plan which may then be 1-2 years old at the time of depo or trial”
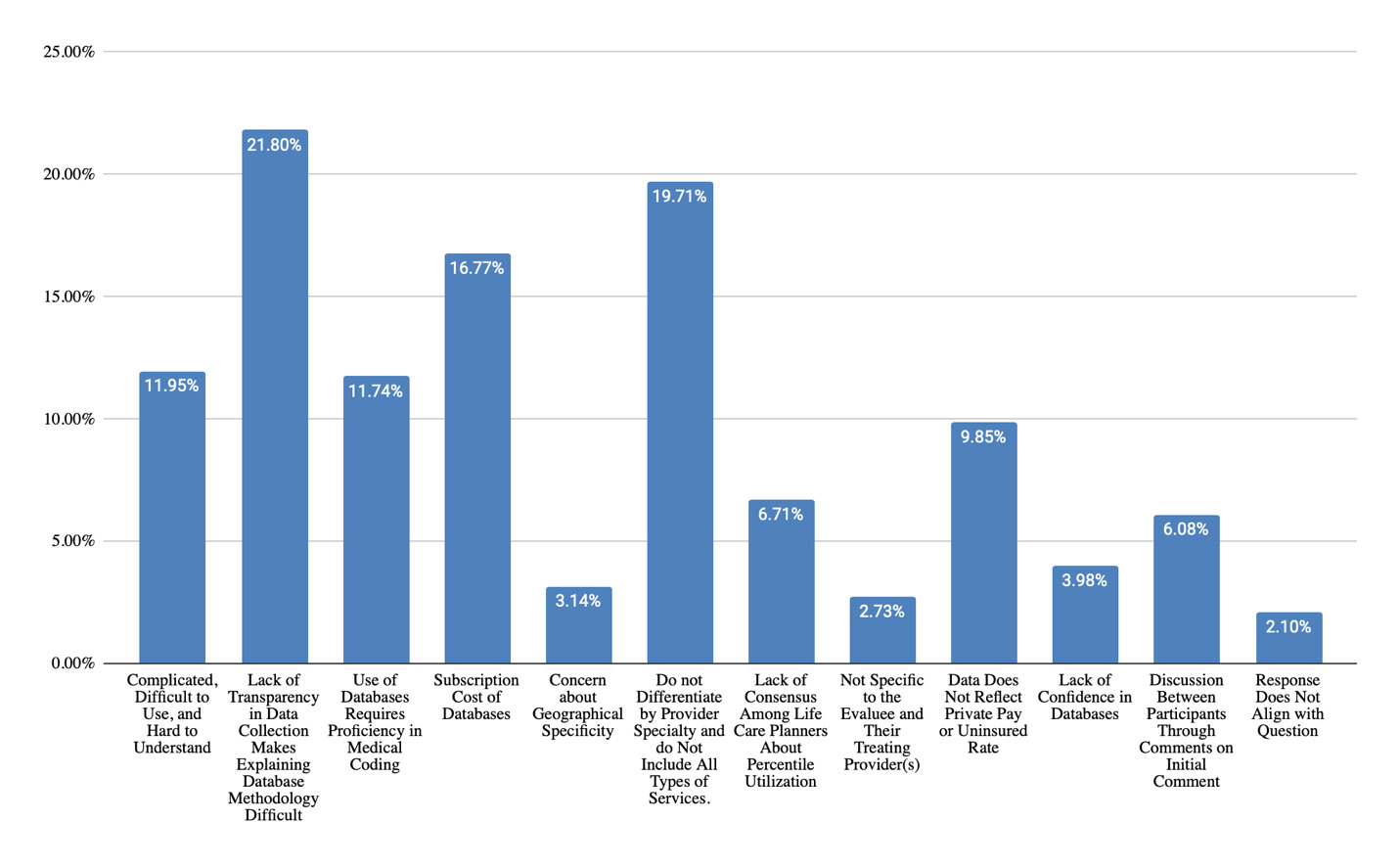
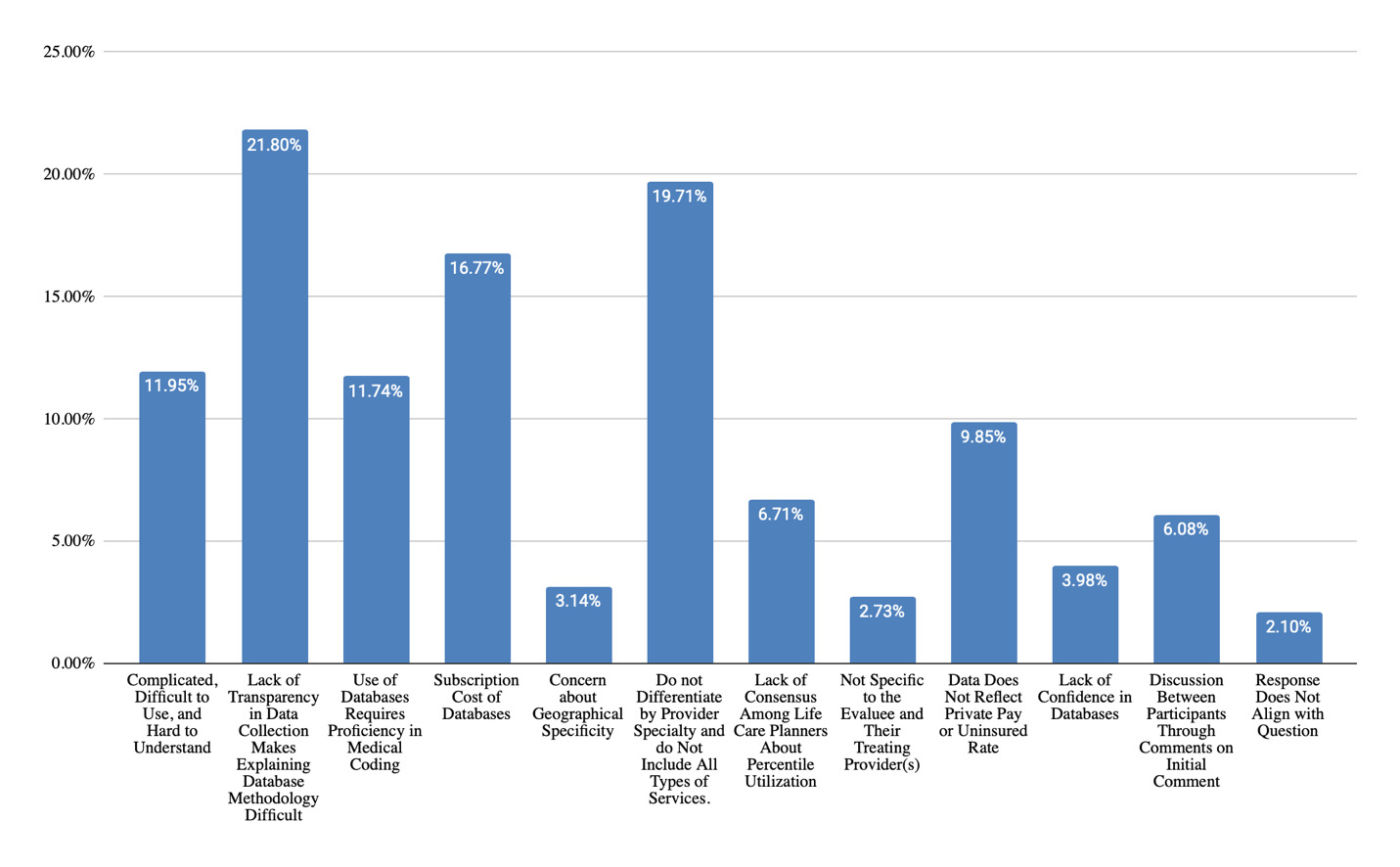
Question 2: “Please discuss the challenges of using paid databases when costing out goods and services within a life care plan (refer to the list of databases provided on screen and mention any specific database you are referring to in your response).”
Themes Identified & Representative Examples
Complicated, Difficult to Use, and Hard to Understand
-
“They can be difficult to access and obtain information if you don’t know what your doing”
-
“A learning curve to use each database”
-
“You have to know how to enter the right data to get what you need”
-
“Some databases are quite complex and difficult to use”
-
“Understanding how to use them correctly”
Lack of Transparency in Data Collection Makes Explaining Database Methodology Difficult
-
“Proprietary data”
-
“Need to understand and explain details about how they collect their data in deposition/trial”
-
“Finding out all of the details regarding their data collection, scrubbing, sources, etc.”
-
“Not publishing the sources for their data”
-
“The specific sources used to gather the data is not available.”
Use of Databases Requires Proficiency in Medical Coding
-
“Knowing all required cpt codes”
-
“You have to ensure correct use and understanding of codes”
-
“Need to be skilled at correct coding, etc.”
-
“Must know comprehensive codes for information being sought”
-
“Need to have the correct CPT codes as some procedures such as scoliosis surgeries have multiple options to choose from”
Subscription Cost of Databases
-
“Cost”
-
“They are expensive to use”
-
“Costs are prohibitive for new businesses”
-
“Some are very expensive for an independent consultant”
-
“Overly expensive”
Concern About Geographic Specificity
-
“Some resources are national or state based, not geographically specific”
-
“If the database doesn’t encompass the state for which you need information”
-
“geographic area may not be adequately represented in more rural areas”
Do Not Differentiate by Provider Specialty and do Not Include All Types of Services
-
“Same costs for different specialists”
-
“Don’t allow for specialty differentiation”
-
“Only some fees are found in the databases; not everything is there”
-
“Does not cover everything you need (long term care, home health, etc.)”
-
“Not everything is in there. Doesn’t allow for the variations in additional costs”
-
“Do not differentiate between generalist and specialty providers.”
Lack of Consensus Among Life Care Planners About Percentile Utilization
-
“Too many life care planners using different percentiles. 50, 75, 90. It leads the LCP group as a whole to look fractured and possibly it might look like it is a guessing game.”
-
“More research is needed”
-
“Have there been any studies regarding if the LCP is appropriately funded at each level? Was there enough money? or did they run out?”
-
“Why can’t we use a range?”
-
“I do not agree with using the 50th percentile. When we are working with people who are catastrophically injured, they need the best care, and eliminating their access to 50% of the providers does not appear to be best practice.”
Not Specific to the Evaluee and Their Treating Provider(s)
-
“Dost not reflective of current providers”
-
“Do not provide access to care for the patient. Physician offices will not honor a database.”
-
“Not necessarily specific to the person”
Data Does Not Reflect Private Pay or Uninsured Rate
-
“Do not tell us what the provider will accept, rather than what is on the bill”
-
“Uses Billed and Charged Data Only, No Reference to what is amount for paid responsibility to the patient is not going through insurance company for payment”
-
“They don’t provide private pay rates which is an obvious option for a life care plan”
-
“They do not include one single datapoint for individuals who are uninsured and/or are paying private pay so are not a true and all inclusive representative of what an individual will expect to pay for services”
Lack of Confidence in Databases
-
“Doesn’t account for a range”
-
“Verifying data”
-
“Doesn’t always incorporate SCS costs included in the hospital fees. Or other equipment supplies”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “Need to understand and explain details about how they collect their data in deposition/trial”
- Response(s): “Agreed.” “Most databases will provide detailed information about how they collect data that you can use in depo or trial”
-
Initial comment: “difficult to sort out outpatient vs ACS”
- Response(s): “Context4Healthcare allows this”
-
Initial comment: “Costs, small practitioners may not be able to afford”
- Response: “also the data bases are not current on the cost of labor which impacts provider” “Firming up the validity of your LCP should be well worth the small investment to obtain reliable and accurate data”
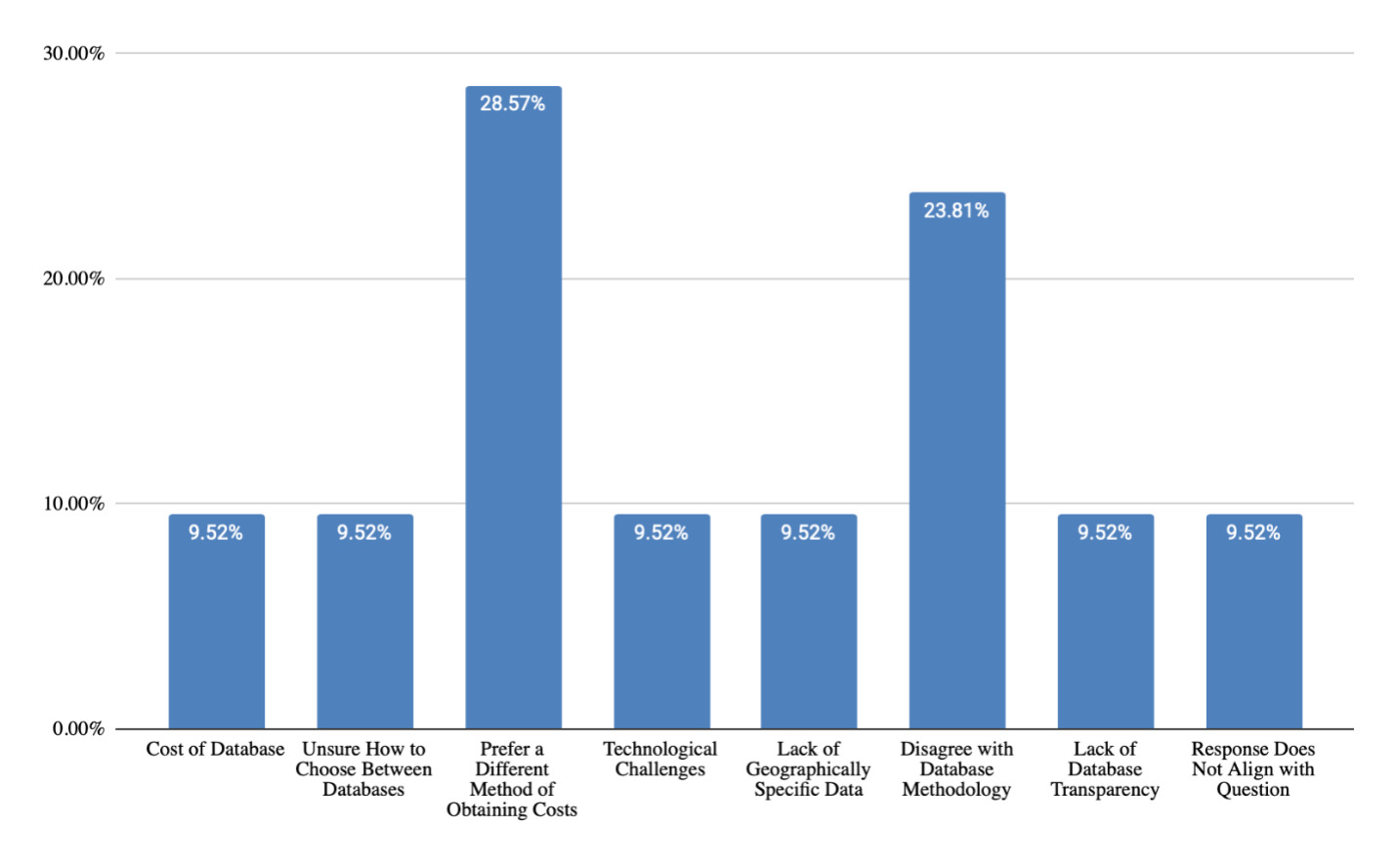
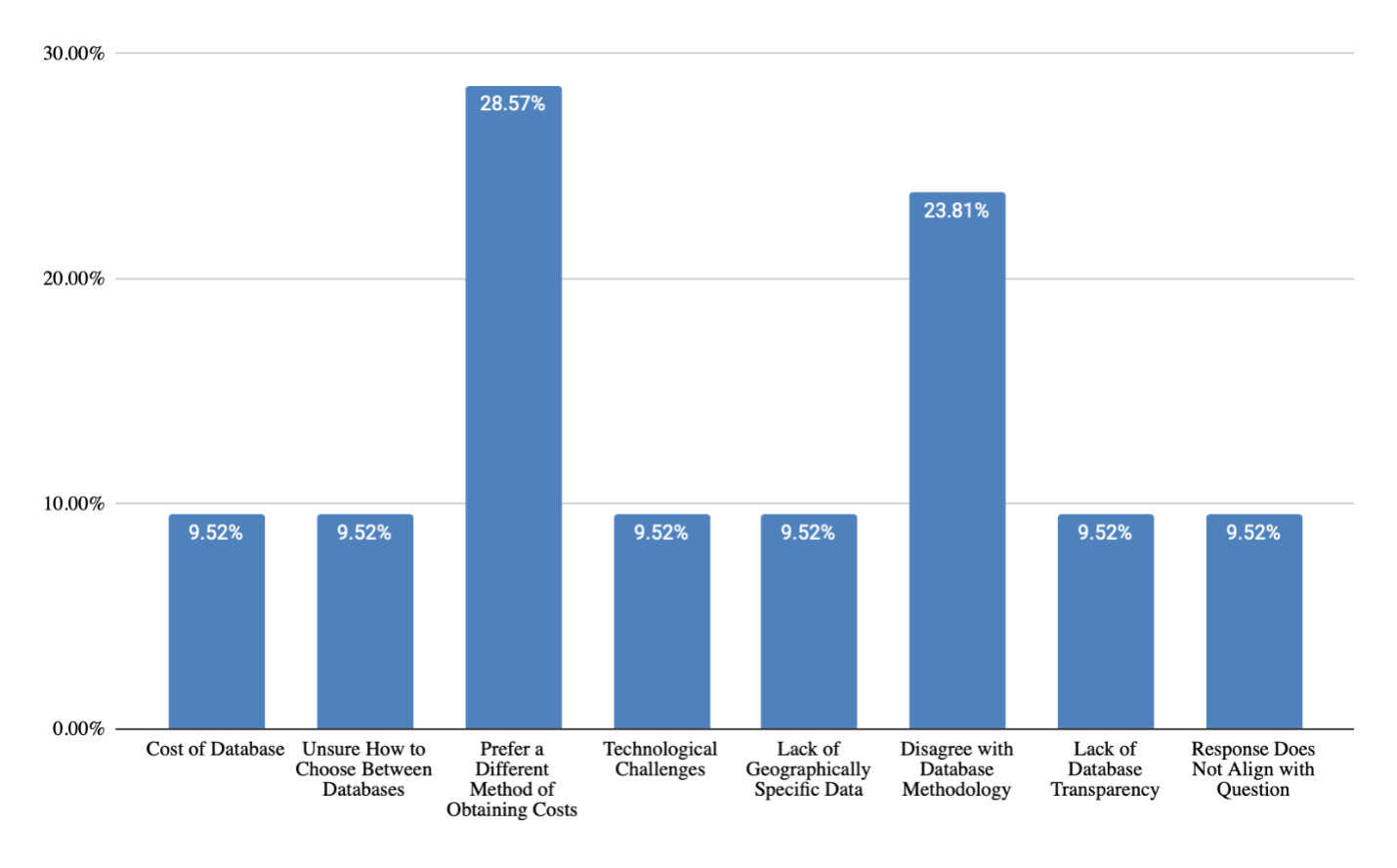
Question 3: “If you do not utilize paid databases as a technique, please explain why.”
Themes Identified & Representative Examples
Cost of Databases
- “I can’t justify the cost. I use some, but not the more costly ones.”
Unsure How to Choose Between Databases
- “Not sure which one to use bec they all seem to have different data.”
Prefer a Different Method of Obtaining Costs
-
“Prefer to use existing bills of providers”
-
“We are able to get real time costs via phone calls”
-
“One thing that we have not discussed is patient right to choose. If patient is established treating with a provider, does he have the right to have the affordability to continue with that provider?”
Technological Challenges
- “Still have a landline!”
Lack of Geographically Specific Data
- “Most do not contain data from the state where I practice”
Disagree with Database Methodology
- “I avoid databases because they do not provide the “reasonable value” or accepted amount for services. If there was such a database, I would use it” “Because they are based on charge data, which is not the type of data that I believe is relevant to fund a LCP.”
Lack of Database Transparency
- Not willing to publish sources
Medical Bills
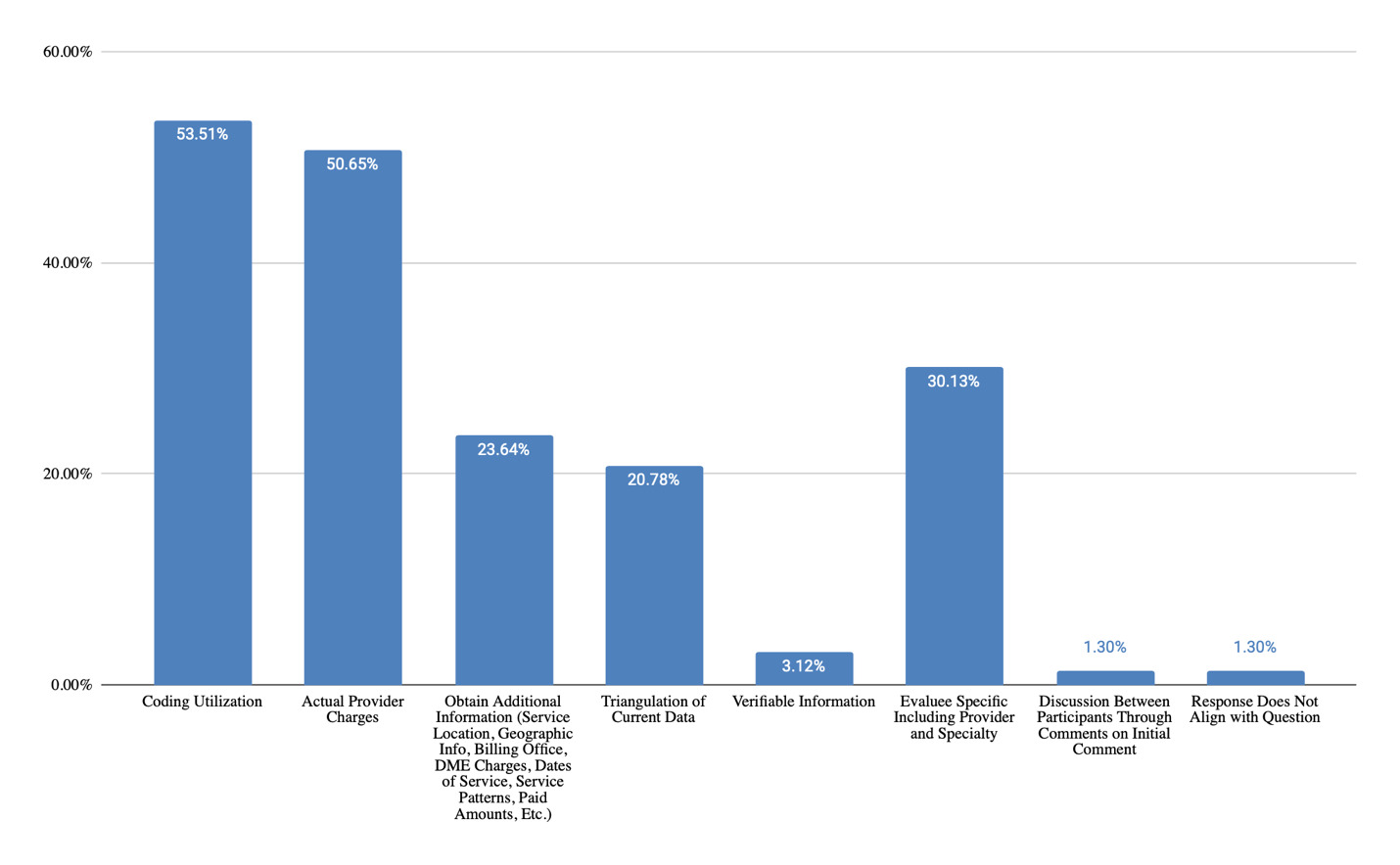
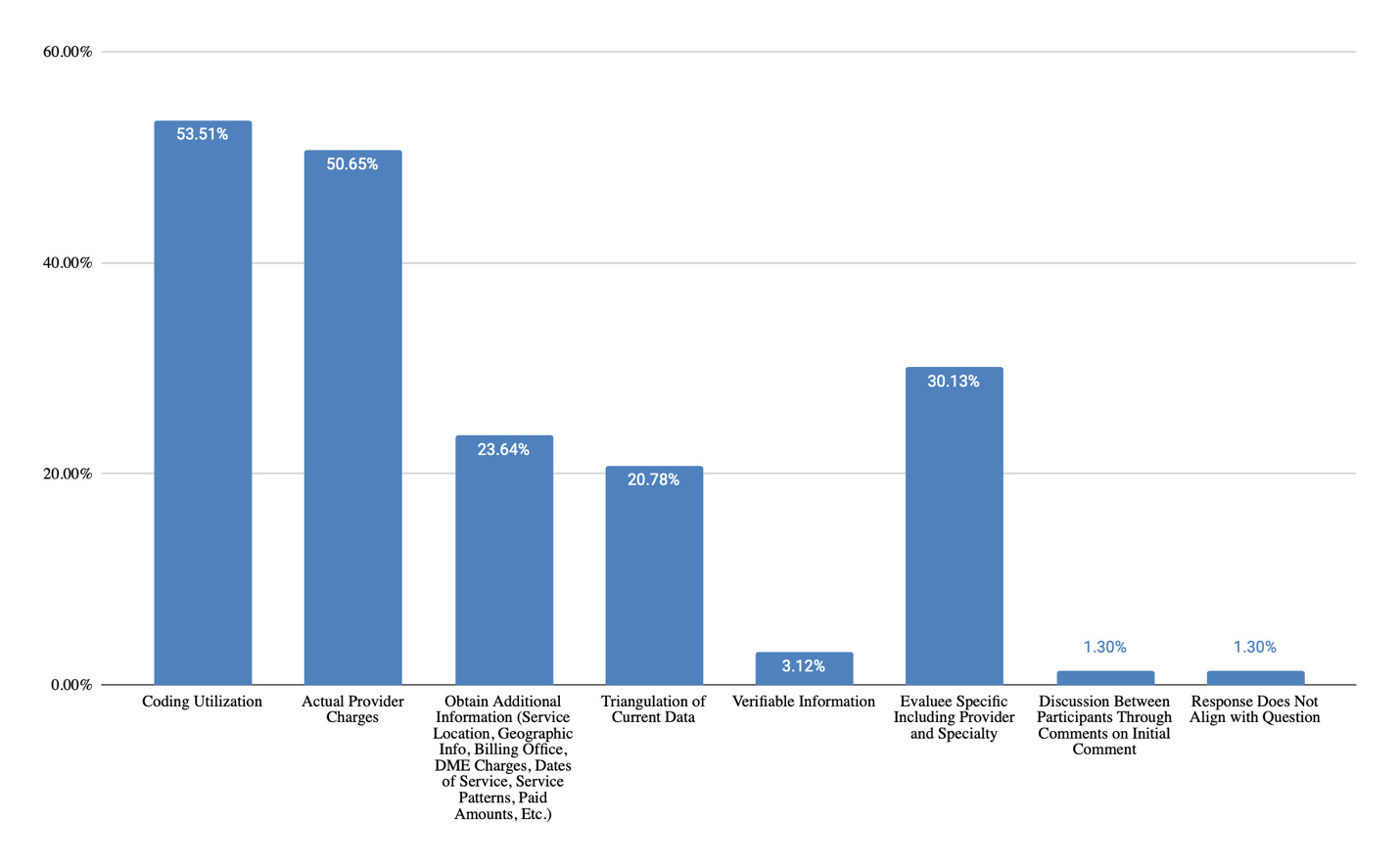
Question 1: “Please discuss the strengths of using medical bills when costing out goods and services within a life care plan.”
Themes Identified & Representative Examples
Coding Utilization
-
“Great source for CPT codes and for comparison data”
-
“You can look at the typical CPT codes used for that individual”
-
“Medical bills provide cpt codes helpful for determining future care”
-
“Can help to identify past cpt codes and patterns of care/services”
-
“Provides the codes necessary for additional pricing analysis”
-
“Helpful if using it for codes for repeat procedure”
Actual Provider Charges
-
“Demonstrates what the provider actually charged for items - hard to dispute that!”
-
“Past charges are a good reflection of charges and represent actual amounts billed”
-
“Actual charge from the actual provider”
-
“They provide a historical understanding of actual charges the patient has incurred, which can be helpful when trying to determine future hospitalizations and typical ER level of complexity”
-
“If current, then represent actual charge(s) from a treater”
-
“Best, most reliable costs - the actual costs”
Obtain Additional Information (Service Location, Geographic Info, Billing Office, DME Charges, Dates of Service, Service Patterns, Paid Amounts, Etc.)
-
“In addition to the actual charges, the bills can offer CPT codes, location of services provided, physician information, billing office to contact, etc. Current billing can offer more than just the actual charges.”
-
"Good for LTC, rehab, fancy wheelchair, and other things that aren’t in databases or “able to be googled.”
-
“Practice patterns for future services”
-
“Set pattern, frequency of treatment”
-
“If you are costing a procedure that you know will happen soon after the LCP is written, then you have accurate data with the patient’s provider/geographical area.”
Triangulation of Current Data
-
“Great source for CPT codes and for comparison data”
-
“Past charges are a good reflection of charges and represent actual amounts billed. This can be compared to data bases and/or calls to other vendors to see where they lie on the cost spectrum.”
-
“Helpful if current year”
-
“Provides good information re. coding for complex issues; reference for pricing; comparative values; practice patterns for future services”
-
“Strengths are it’s a resource you can use along with others. Triangulation”
-
“If costs are from the last 6 months, then you can use them as one cost.”
Verifiable Information
-
“Verifiable information”
-
“Can verify codes and cost provider to the client by thier treating provider.”
-
“Verifiable information with actual charges”
Evaluee Specific Including Provider and Specialty
-
“You can look at the typical CPT codes used for that individual.”
-
“They provide the CPT codes used by the specific provider for sourcing and individualized for the evaluee.”
-
“Actual charge to or for the individual”
-
“Evaluee specific”
-
“Specific to the evaluee, reliable data for the specific individual”
-
“It is the only charged amount that is actually true to the client and service”
-
“It is actual charge specific to the individual”
-
“There may be some specific codes that the patient requires along with a procedure, etc.”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “patient specific; for surgeries/procedures, all codes/costs are accounted for; its the treater”
- Response: “very few people have the same surgeries over and over so not sure what this means”
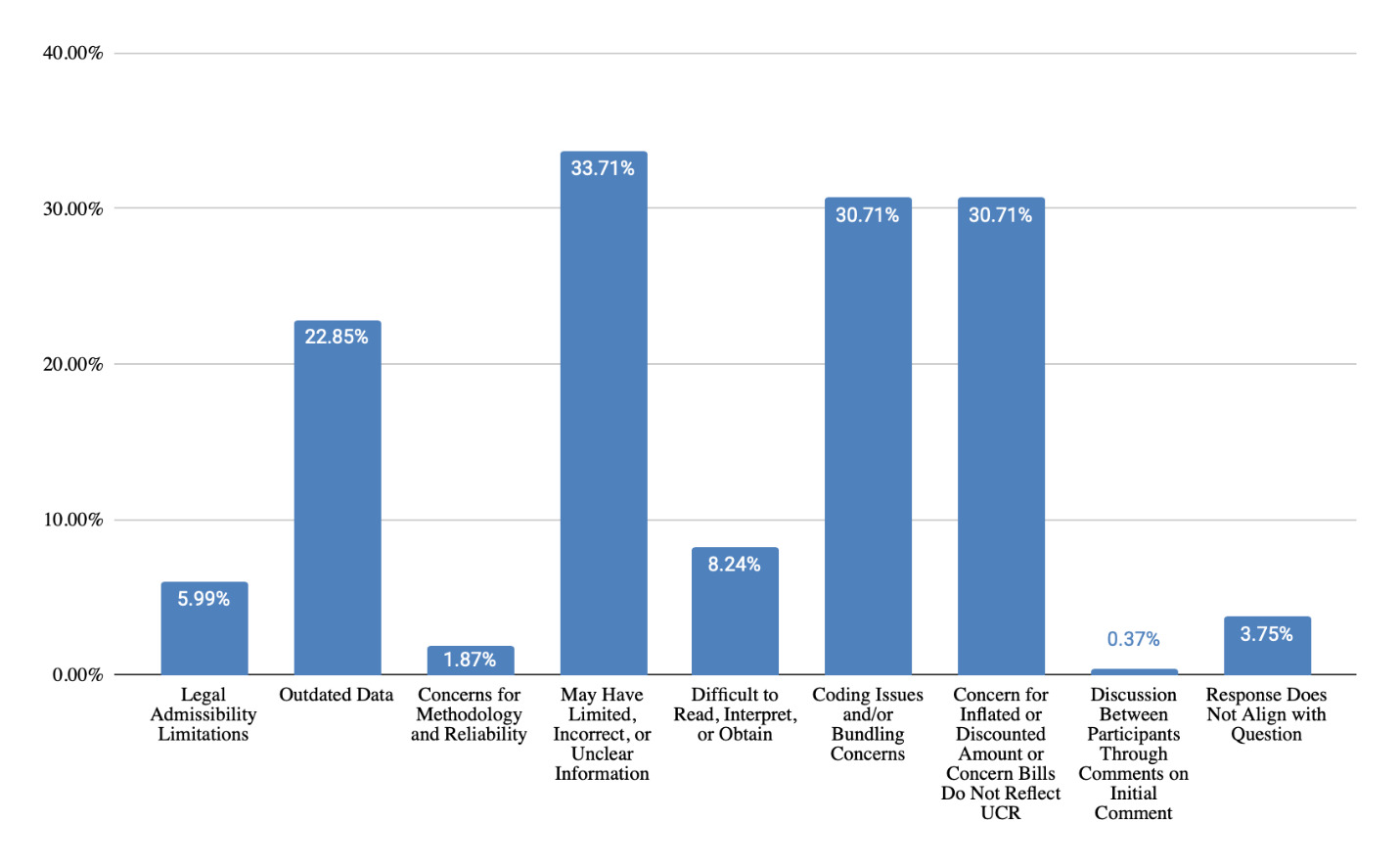
Question 2: “Please discuss the challenges of using medical bills when costing out goods and services within a life care plan.”
Themes Identified & Representative Examples
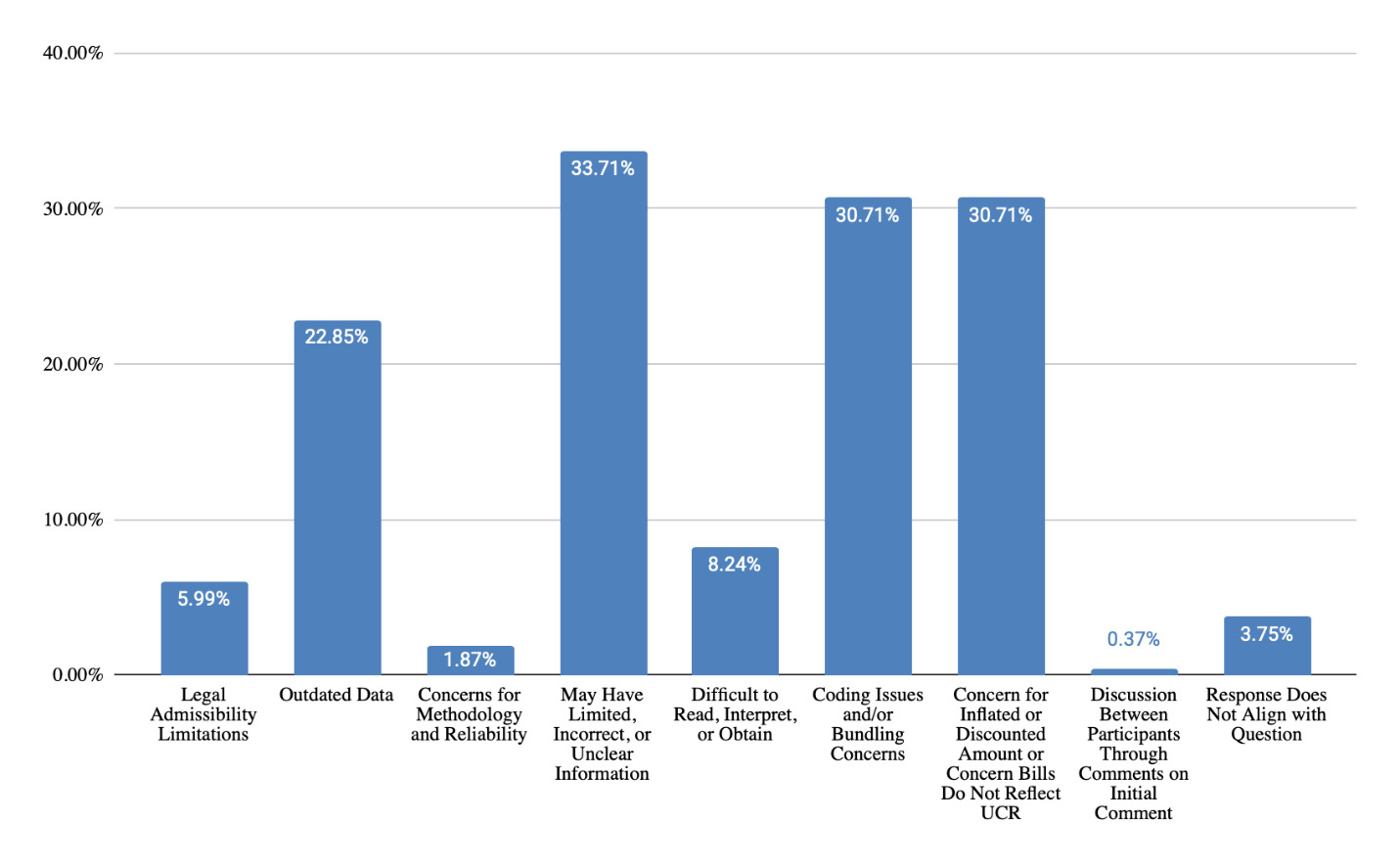
Legal Admissibility Limitations
-
“Not allowed to be relied upon in CA / Correnbaum”
-
“Does it stand up to litigation.?”
-
“Howell and Corenbaum rulings in California”
-
“They are case specific, which is a no-no.”
Outdated Data
-
“Historical data and not projective of future costs”
-
“Not up to date”
-
“Not current costs, sometimes years old.”
-
“One bill by one provider at one time in past.”
Concerns for Methodology and Reliability
-
“Not enough data points to show scientiffc method”
-
“Fees utilized are for insurance submission or collateral source submission”
May Have Limited, Incorrect, or Unclear Information
-
“Does not always tell the ‘whole story’”
-
“We don’t always know if the coding is correct to reuse for future costing purposes.”
-
“N=1”
-
“Costing information is limited to one provider instead of many providers within a database.”
Difficult to Read, Interpret, or Obtain
-
“Understanding them”
-
“Photocopied bills can be difficult to read. They can be extremely repetitive.”
-
“They are not always easy to obtain”
-
“Legibility can be difficult.”
Coding Issues and/or Bundling Concerns
-
“Accuracy of CPT codes, bundled services.”
-
“CPT codes utilized may not be used in future.”
-
“Bills could be erroneous or unbundled.”
-
“For future surgery with another provider will it be the same coding ?”
Concern for Inflated or Discounted Amount or Concern Bills Do Not Reflect UCR
-
“Bill charges does not always reflect UCR.”
-
“Particular physicians especially those who do the procedures or injections in their facility or have ownership in the surgical facility often bill a largely inflated rate”
-
“In my opinion they are third party negotiated rates and therefore I do not use them. They do not indicate to me what the cost is to the person for same service in the future absent collateral source payer etc.”
-
“Not always a true or accurate reflection of what a person will be expected to pay for services after litigation. Many times providers that are ‘not retained’ experts/treaters charge high charges so that the settlement for past medical will be astronomically high, but then after the case has settled they will accept much less than what was reflected in the past bills.”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “It should not be used as a sole source for costing. CPT codes utilized may not be used in future.”
- Response: “yes but if that cpt code is deleted or amended the future code books will have a cross walk for it”
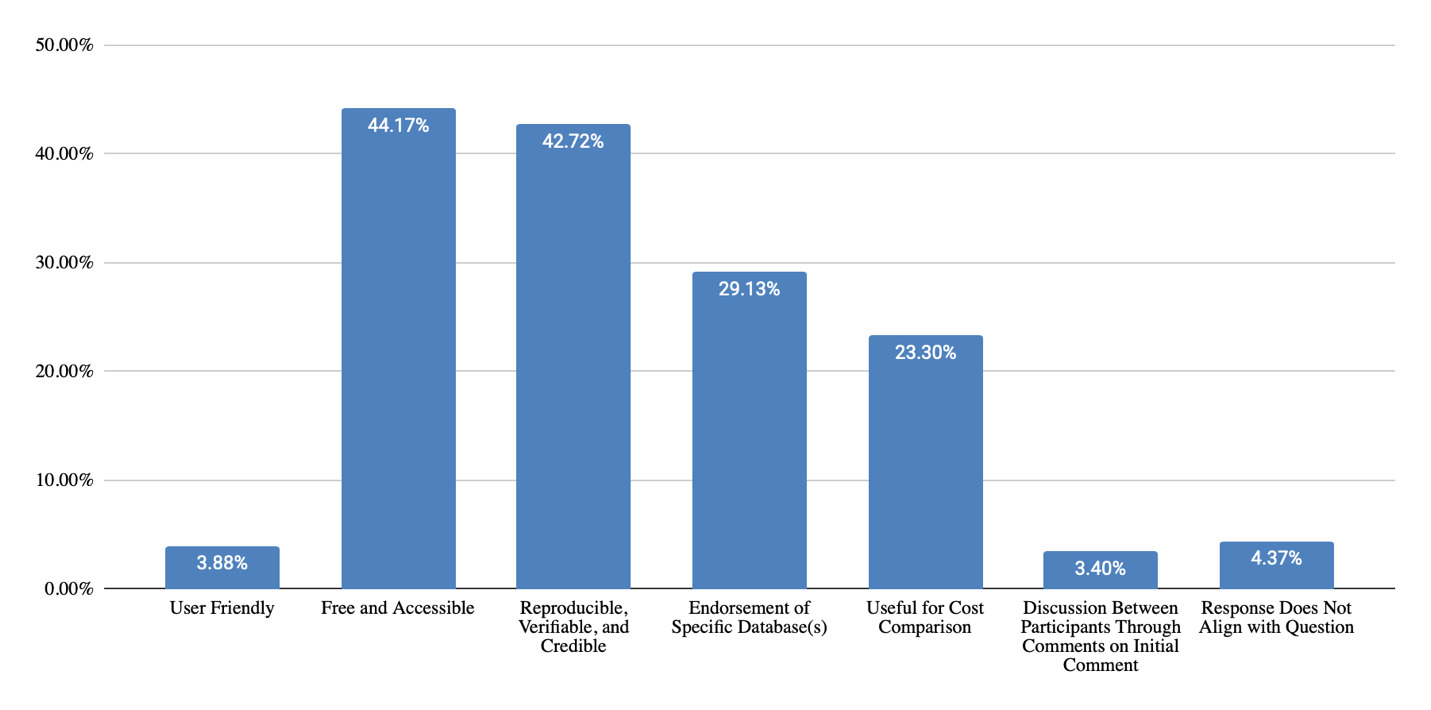
Free/Open Access Databases
Question 1: “Please discuss the strengths of using free or open access databases when costing out goods and services within a life care plan (refer to the list of databases provided on screen and mention any specific database you are referring to in your response).”
Themes Identified & Representative Examples
User Friendly
-
“Relative ease of use…”
-
“Another resource simple to use.”
-
“Simple to use and mostly verifiable”
Free and Accessible
-
“No associated costs or requirement of contract for obtaining costs.”
-
“They are free.”
-
“Free easy access.”
-
“Consistent, free and easily available to the public.”
-
“They are available to all life care planners.”
Reproducible, Verifiable, and Credible
-
“Verify through contact with those providers”
-
“Easy to reproduce”
-
“Easily verifiable”
-
“Mostly verifiable”
-
“Hundreds and thousands of data points.”
-
“The ones sponsored by a government agency… garner credibility.”
-
“Accessibility to everyone for reproducibility”
-
"Can be replicated
Endorsement of Specific Database(s)
-
“GoodRX provides good medication info, but not all meds”
-
“When government supported and verified it has the strength of all those resources behind it and provides defensible data; such as VA Reasonable Charge Data”
-
“The va has a conversion factor that allows for specialty modification.”
-
“CMS.data.gov provides physician charges for evaluation and management codes. VA data is a reliable governmental resource.”
-
“No charge for goodrx, but that is the only reliable free database to use consistently within a LCP.”
-
“Good rx, cosumer fair ehalth for codes”
Useful for Cost Comparison
-
“Can locate local pricing for services such as housekeeping, lawn care, etc. and verify through contact with those providers”
-
“Good resource for comparative pricing.”
-
“It is possible to see what the consumer might see and compare it with actual billings or with paid subscription data.”
-
“Verifiable tool for Triangulation”
-
“It gives you another resource to use when triangulating.”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “no charge for goodrx, but that is the only reliable free database to use consistently within a LCP.”
-
Response: “GoodRx says on their website that the costs are discounted. How can this data be acceptable according to our standards.”
-
Response: “Not true”
-
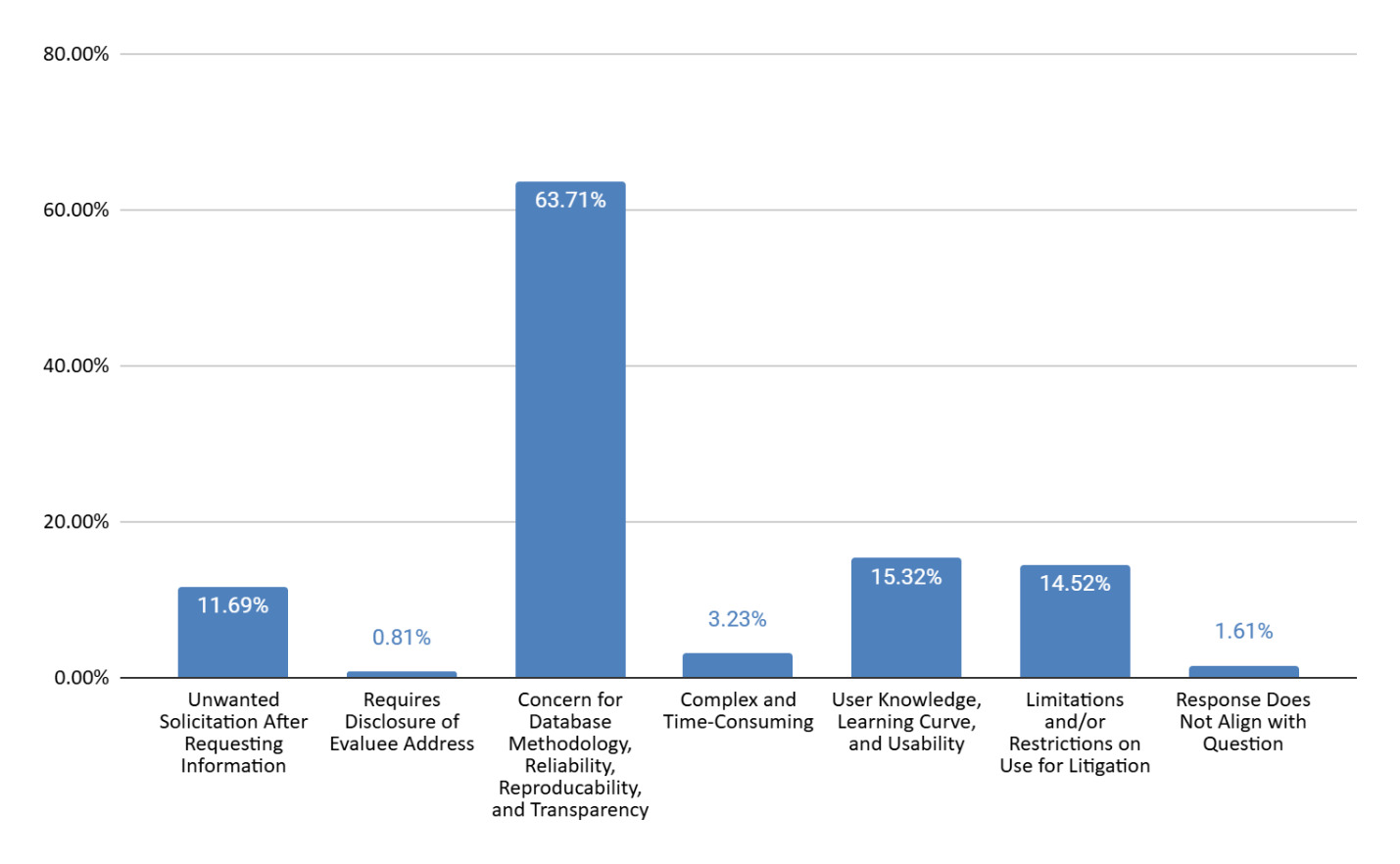
Question 2: “Please discuss the challenges of free or open access when costing out goods and services within a life care plan (refer to the list of databases provided on screen and mention any specific database you are referring to in your response).”
Themes Identified & Representative Examples
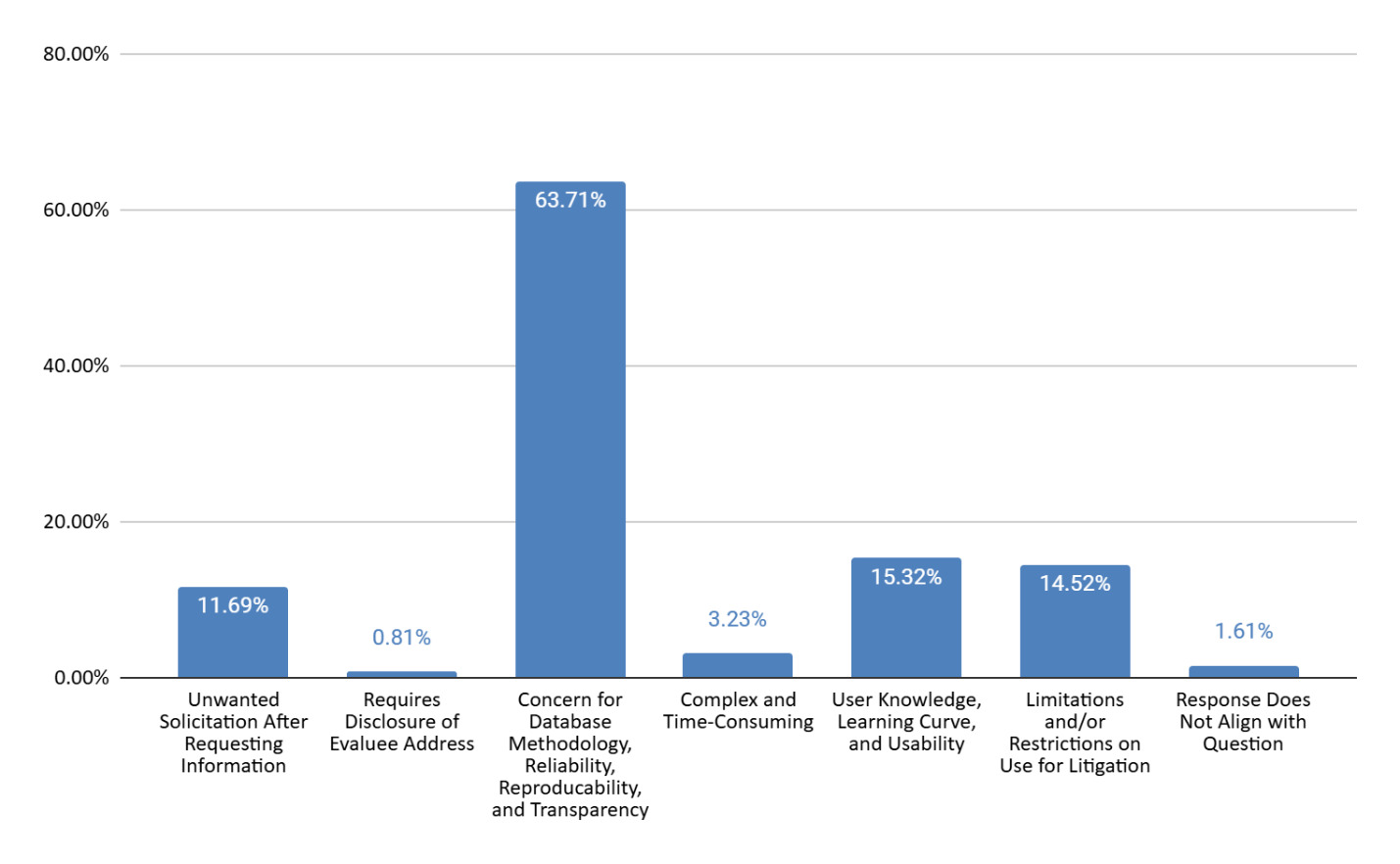
Unwanted Solicitation After Requesting Information
-
“If considering a Place for Mom or angie’s list as a data base per se, the issue is then the companies will call and email me for days on end for months to see if i am going to hire them…you have to give your info on their website in order to get the info. One is i feel bad i am not acutally giving them the business and the second issue is i am annoyed by the contacts.”
-
“They want your personal info so they can call you, I don’t want sales calls”
-
“They call you forever after”
Requires Disclosure of Evaluee Address
-
“Needing to give a specific address for services such as lawn care”
-
Concern for Website Methodology, Reliability, Reproducability, and Transparency
-
“Unsure how they got their data (some of them).”
-
“May not know the sources of where they get the info”
-
“Unsure of reliability, lack of transperancy”
-
“Not always reproducible”
Complex and Time-Consuming
-
“VA is complicated and you need to understand the different tables and which to use”
-
"Can be complicated to calculate (e.g., VA info).
-
VA Database is time consuming."
User Knowledge, Learning Curve, and Usability Challenges
-
“Learning curve.”
-
“The user not know how to use it, does not analyze, or understand the source of the data.”
-
“User error.”
-
“Need to get familiar with them to know their limitations and correct use in your analysis.”
Limitations and/or Restrictions on Use for Litigation
-
“Many note that the information is not to be used in litigation settings and state for Consumer Use Only. Ability to replicate with actual service providers.”
-
“Issue if it can be used for commercial purposes.”
-
“Fair Health Consumer - presents different data than the subscription. Can be confusing.”
Preparing for Testimony
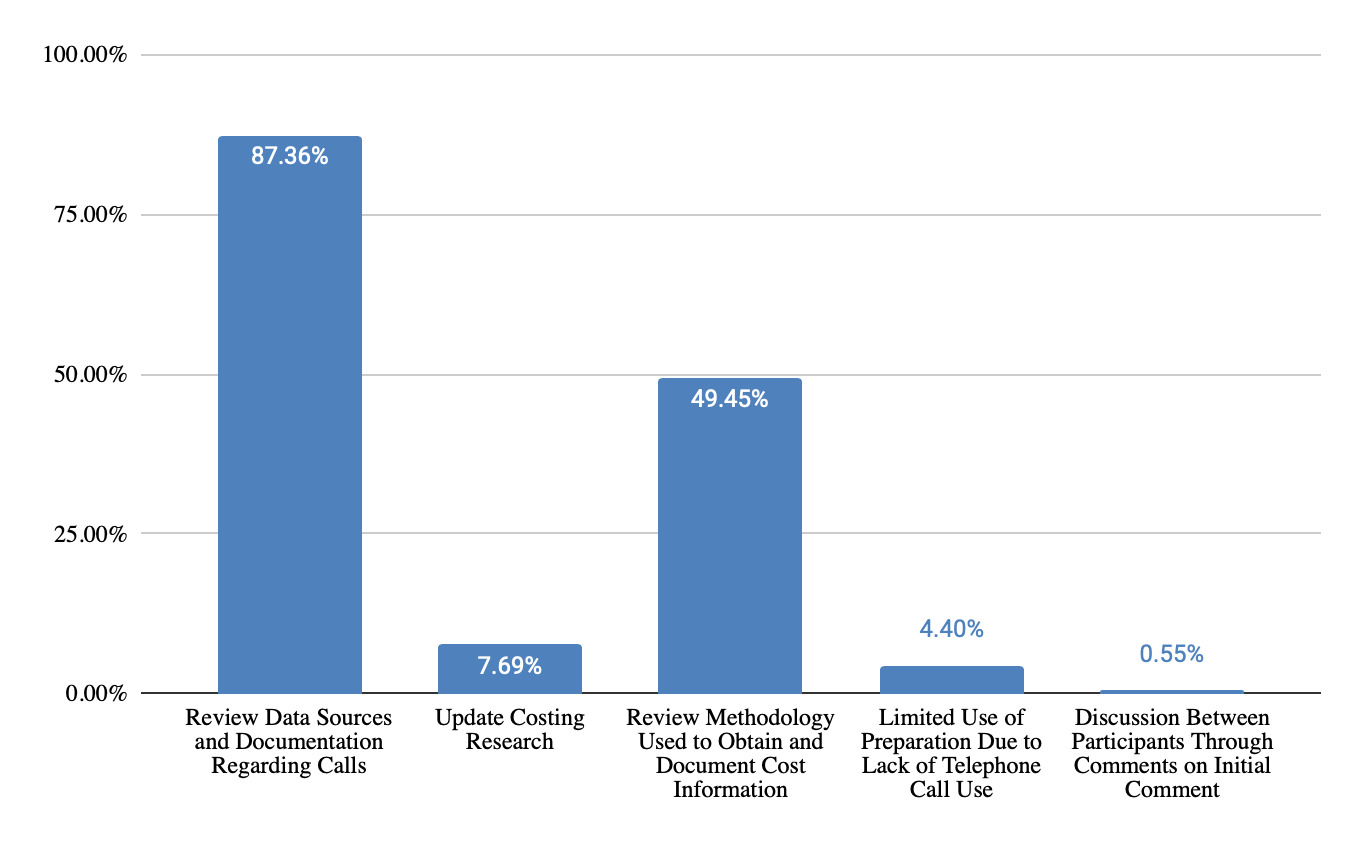
Question 1: “What information do you have prepared regarding telephone costing techniques before testifying?”
Themes Identified & Representative Examples
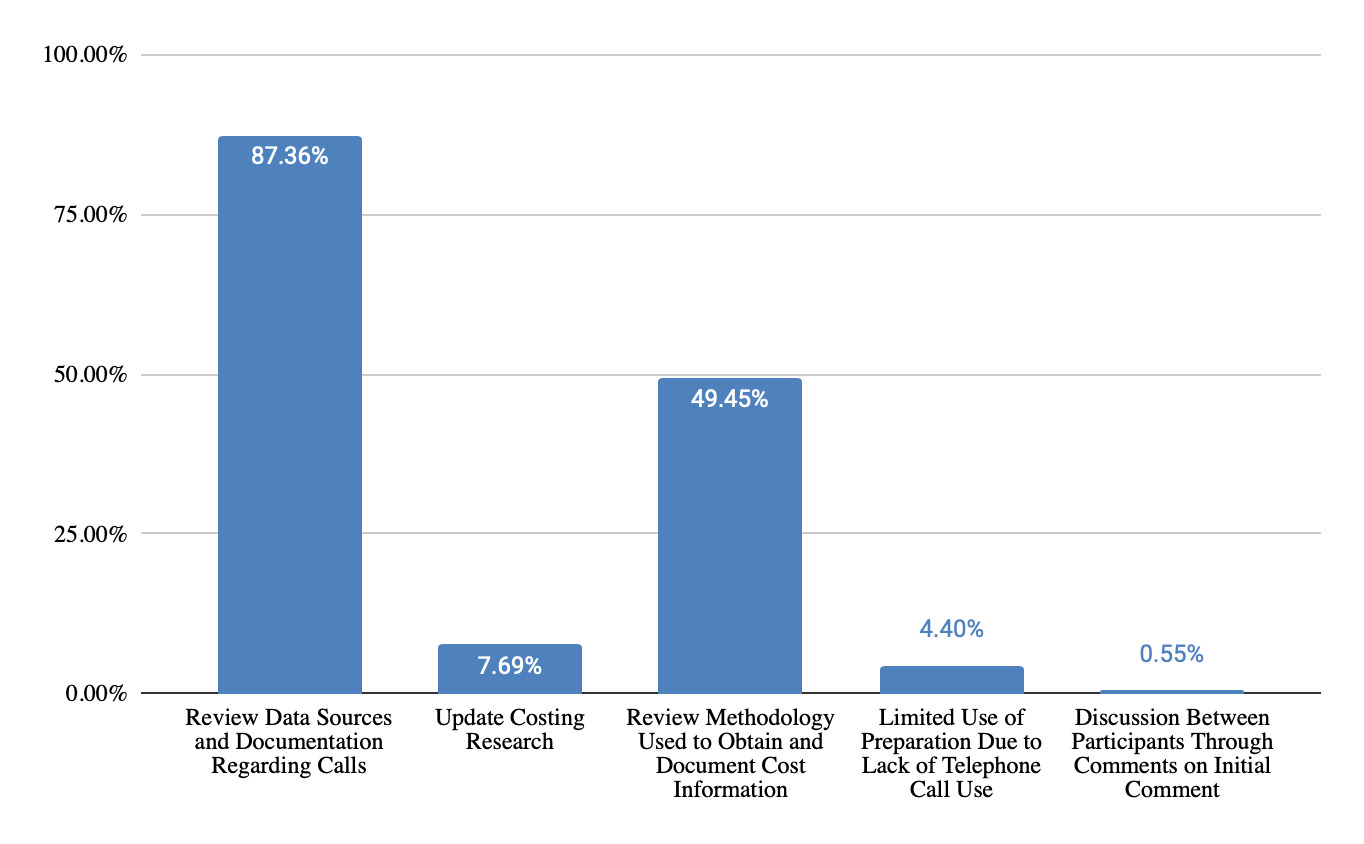
Review Data Sources and Documentation Regarding Calls
-
“Documentation of who I spoke with, date, contact information and any confirmatory emails, rate sheets or other info that has been sent to me”
-
“Company, address, phone, contact person, script, response, date”
-
“Name, phone number, location, contact, date and info provided”
-
“Life Care Plan Research Sheet for each item. Name of item or service, ventor called, contact cost quoted, date of research, name of researcher, geographic location. Printed sugical estimates received from treaters”
Update Costing Research
-
“Update contacts. If older than a year, do updated research and pricing.”
-
"I may call sources again and update costs if it has been a while since costs obtained.
Review Methodology Used to Obtain and Document Cost Information
-
“WHY it was a telephone call versus database, etc.”
-
“What methodology was used to get the phone numbers”
-
“I review my report to make sure that the foundation to support my opinion is referenced and documented”
-
“I have developed a questionnaire to complete while on the phone (name, phone #, date of contact, business name, Question(s) to ask etc.)”
-
“I have a list of all the phone calls that were made, the treating entity, the phone number, the name of person who provided information, date information obtained and detailed information on the costs and any appropriate additional information such as typical frequency of follow-up, or what is included in a per diem rate”
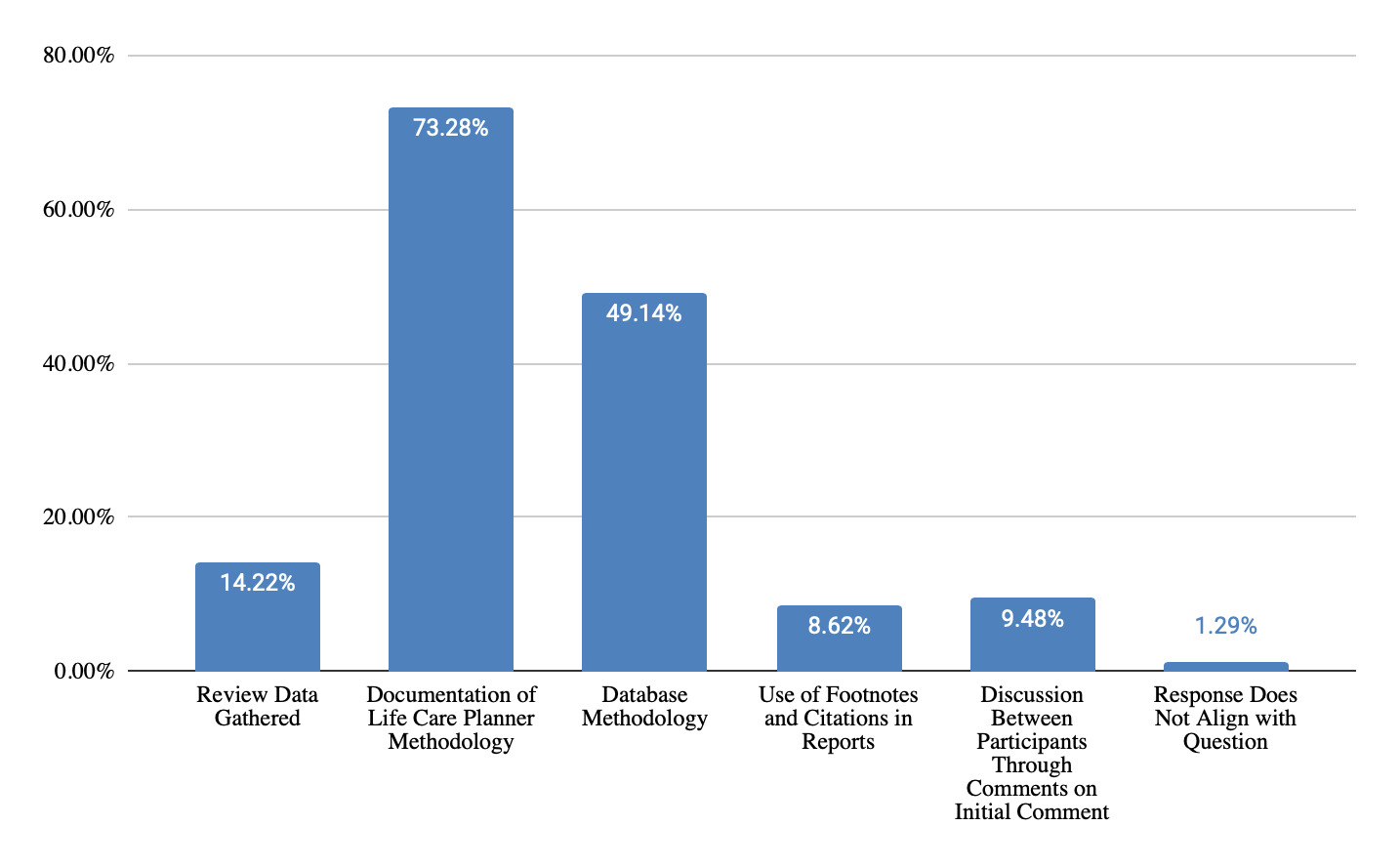
Question 2: “What information do you have prepared regarding database costing techniques before testifying?”
Themes Identified & Representative Examples
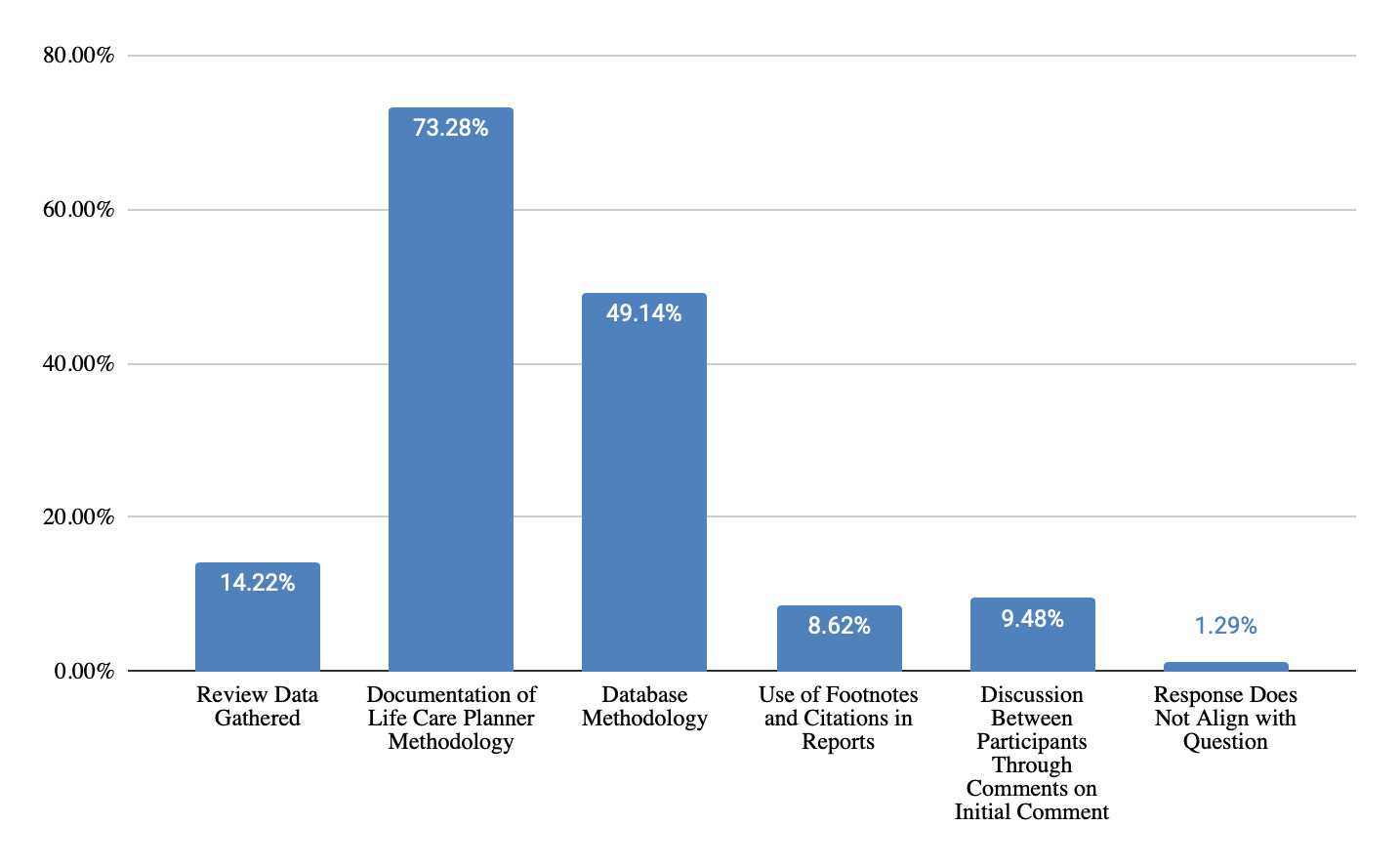
Review Data Gathered
-
“Review Excel Spreadsheets and be able to explain costs and how they were amounted”
-
“Review the printed database documentation, make sure the codes and cost are correct and the correct percentiles are used”
-
“Review my notes…”
-
“Look over my grid…”
Documentation of Life Care Planner Methodology
-
“…Make sure I have screenshot of the costs that I obtained, figure out how to articulate why I used the percentile that I chose.”
-
“The title of the database; references that discuss that database…”
-
“Research file that includes names of database, initials of data analyst, date of data acquisition, CPT/DRG codes, short description, professional vs facility fee and median of cost data obtained.”
-
“…Percentile used for each source, screen shots of each procedure fees”
Database Methodology
-
“Name of database, from where the information in the database was derived…”
-
“Sources used, where data is gathered from each source…”
-
“The methodology use by the database re where the claims data come from and the number ; be able to explain why it is valid and reliable”
-
“Background information of the database and how they acquire the information”
-
“I review the database’s methodology”
-
“Review brief explanation of the resource and its data points, methodology etc. So that I can speak to it intelligently.”
Use of Footnotes and Citations in Reports
-
“Review my… footnotes, and citations in my life care plan. It’s all there!”
-
“Footnote database in report…”
-
“I footnote the report re: where the cost came from.”
-
“Sources footnoted in report and or a separate source list”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “How are folks handling the fact that Fairhealth does not allow use of its data for federal cases?”
-
Response: “You can get special permission from Fair Health. they would have to revise your contract. It was mentioned yesterday during the Fair Health presentatiion”
-
Response: “I thought this was allowed on a case by case basis”
-
Response: “Don’t use it as a source.”
-
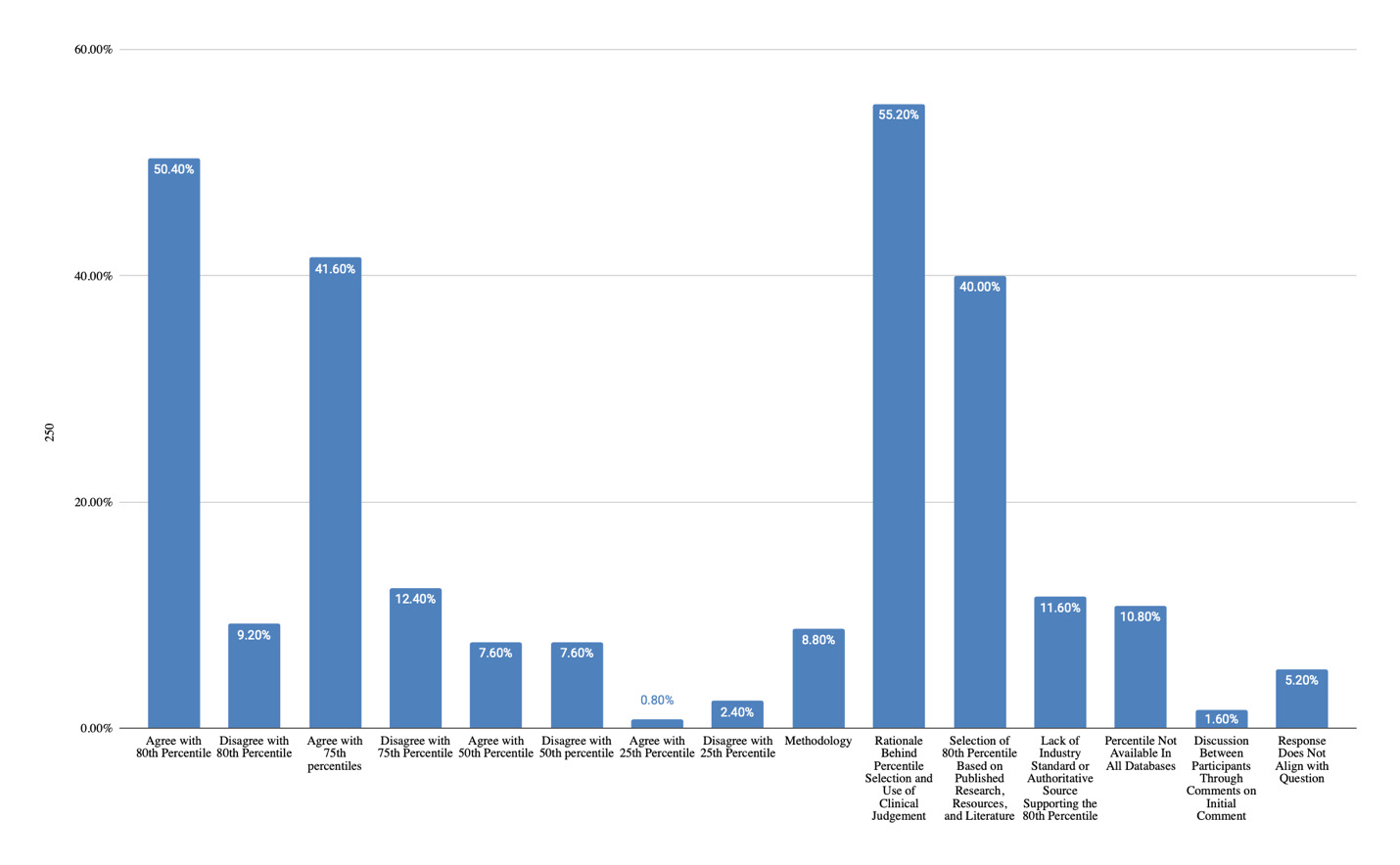
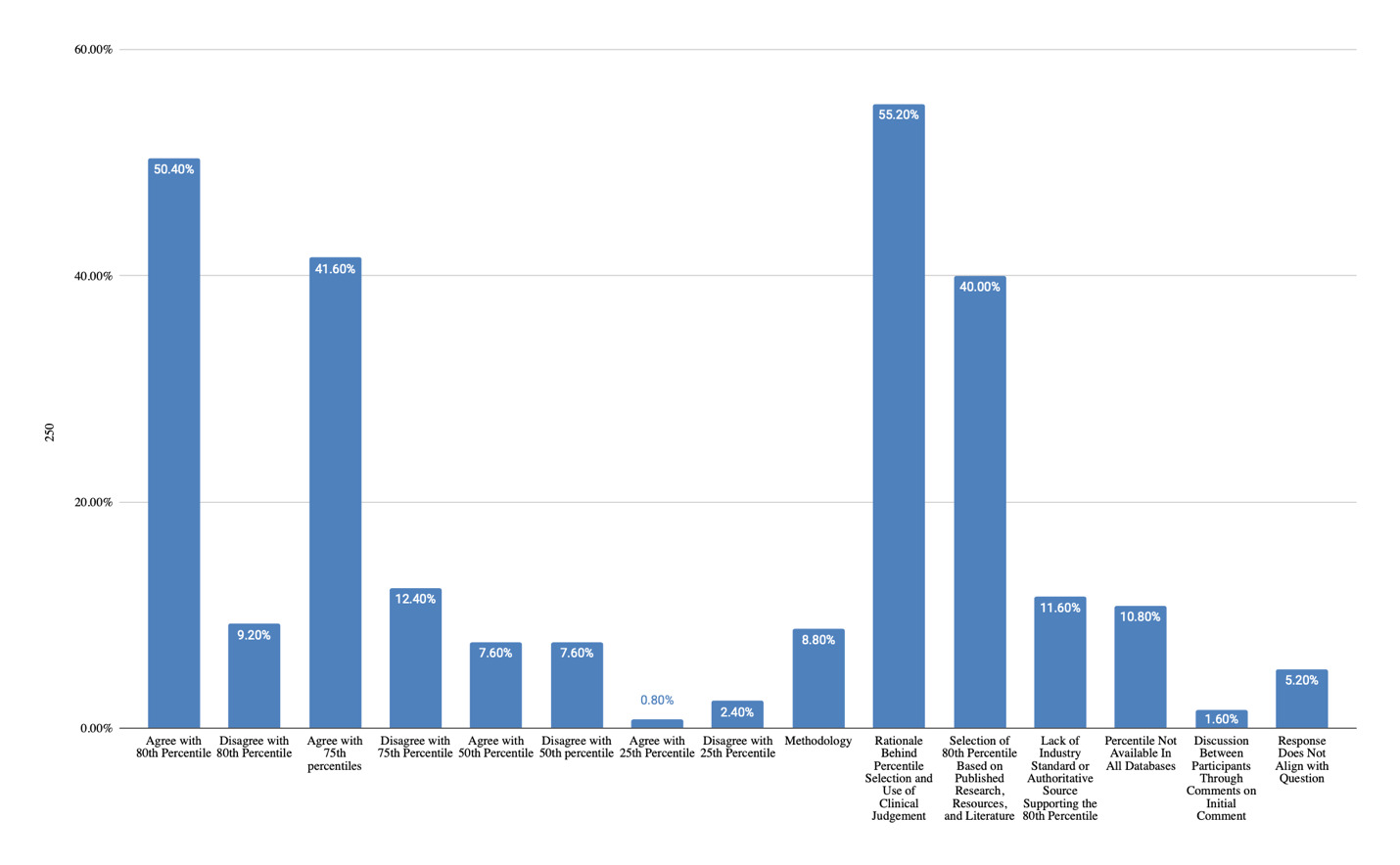
Question 3: “Please discuss the use of the 80th percentile as opposed to 75th, 50th, or 25th percentile as your industry standard when costing?”
Themes Identified & Representative Examples
Agree with 80th Percentile
-
“Generally use 80th percentile as it often aligns with range of costs (mean) obtained from phone calls from actual treating providers.”
-
“I feel the VA is a strong resource and they use the 80th. It is in the federal registry.”
-
“This is a reasonable percentile based on my experience and use of available comparative resources.”
-
“I do not like the concept of excluding 50% of providers as a choice of care for the patient for whom the LCP is created when using 50%tile. I think 75-80%ile is more realistic.”
-
“The the 80th percentile is more likley to allow the disabled person to have services with providers he chooses or is referred to.”
-
“There is consistent references that recommend the use of 75-80th percentile”
-
“Using 75/80 due to published literature”
-
“75th-80 percentile is used by The VA, FairHealth etc. 50th percentile indicates that the evaluee will be excluded from 50% of all service providers in the area.”
-
“80% will only preclude 20% of the service providers from the patient after trial”
-
“It is the prevailing rate per multiple resources and studies.”
Disagree with 80th Percentile
-
“I do not believe it is an accurate number to use.”
-
“It’s not an accurate representation for all services”
Agree with 75th Percentile
-
“Weed, 4th edition - 75th - 80th”
-
“The use of 75-80% percentile is referenced in the life care plan handbook, 4th edition as a common and acceptable practice in the field of life care planning. Costing services at these percentile(s) ensures the evaluee will have access adequate access to medical care and related services.”
-
“It is the prevailing rate per multiple resources and studies. 75th is similar and often the only one available in a database which would also be appropriate. 25th percentile is entirely too low and would not properly provide for the patient.”
-
“I use 75-80 percentile and reference several documents that cite reasoning for pricing with that”
-
“I do not like the concept of excluding 50% of providers as a choice of care for the patient for whom the LCP is created when using 50%tile. I think 75-80%ile is more realistic.”
-
“There is consistent references that recommend the use of 75-80th percentile”
-
“Using 75/80 due to published literature”
-
“75th-80 percentile is used by The VA, FairHealth etc. 50th percentile indicates that the evaluee will be excluded from 50% of all service providers in the area.”
Disagree with 75th Percentile
- “We just recently changed from 75th to 50th percentile.”
Agree with 50th Percentile
-
“The 50th percentile is more probable and closest to actual paid amount”
-
“The 50% does not stop people from using any providers.”
-
“I most often find that the 50% is closed to the self-pay rate.”
-
“Based on stats classes I took the 50th percentile seems more easily defensible.”
-
“The 50th percentile is more probable and closest to actual paid amount”
Disagree with 50th percentile
-
“Just above 50th would address reasonably probable to locate in the market. 75th and 80th percentile is noted by various states, lcp treatise, and other research as UCR. A range between the two points seems reasonable to include.”
-
“I do not like the concept of excluding 50% of providers as a choice of care for the patient for whom the LCP is created when using 50%tile. I think 75-80%ile is more realistic.”
-
“75th-80 percentile is used by The VA, FairHealth etc. 50th percentile indicates that the evaluee will be excluded from 50% of all service providers in the area.”
-
“References recommend using 75-80%. 50% is too low and does not reflect the industry standard especially for specialized providers.”
Agree with 25th Percentile
- “WE use the standard 50th, 75th, or 25th.”
Disagree with 25th Percentile
- “25th percentile is entirely too low and would not properly provide for the patient.”
Methodology
-
“I think it is most important is to use the same percentile in each plan and be able to defend the reason why. Stick with your methodology.”
-
“As long as you pick one and use it consistently and are able to provide a reasonable foundation for why it is used you should be good. Just be consistent and have an understanding of why you use it and have an explanation ready.”
Rationale Behind Percentile Selection and Use of Clinical Judgement
-
“Use percentile consistent or close to what I know the community charges are as a baseline.”
-
“I most often find that the 50% is closed to the self-pay rate.”
-
“Based on stats classes I took the 50th percentile seems more easily defensible.”
-
Selection of 80th Percentile Based on Published Research, Resources, and Literature
-
“Weed, 4th edition - 75th - 80th”
-
“I review that UCR according to multiple sources relied upon by other life care planners to be between the 7th-80th”
-
“The use of 75-80% percentile is referenced in the life care plan handbook, 4th edition as a common and acceptable practice in the field of life care planning. Costing services at these percentile(s) ensures the evaluee will have access adequate access to medical care and related services.”
-
“There is consistent references that recommend the use of 75-80th percentile”
-
“Using 75/80 due to published literature”
-
“References recommend using 75-80%. 50% is too low and does not reflect the industry standard especially for specialized providers.”
-
“75th-80 percentile is used by The VA, FairHealth etc. 50th percentile indicates that the evaluee will be excluded from 50% of all service providers in the area.”
Selection of 80th Percentile Based on Published Research, Resources, and Literature
-
“Is the percentile now used by most states for dispute resolution”
-
“The VA Reasonable Charge Data utilizes the 80 percentile as a reasonable amount and other entities accept that as payment. It is the prevailing rate in insurance for out of network charges”
-
“NY state specifically refers to the 80th for Out of Network Reimbursement via Fairhealth”
-
“80% percentile is well documented in the peer-review literature . Some databases do not have the 80th - in those cases use the 75th percentile.”
-
“It is the prevailing rate per multiple resources and studies. 75th is similar and often the only one available in a database which would also be appropriate. 25th percentile is entirely too low and would not properly provide for the patient.”
-
“I use 75-80 percentile and reference several documents that cite reasoning for pricing with that”
-
“Just above 50th would address reasonably probable to locate in the market. 75th and 80th percentile is noted by various states, lcp treatise, and other research as UCR. A range between the two points seems reasonable to include.”
-
“Weed, 4th edition - 75th - 80th”
-
“The use of 75-80% percentile is referenced in the life care plan handbook, 4th edition as a common and acceptable practice in the field of life care planning. Costing services at these percentile(s) ensures the evaluee will have access adequate access to medical care and related services.”
-
“There is consistent references that recommend the use of 75-80th percentile”
-
“Using 75/80 due to published literature”
-
“I feel the VA is a strong resource and they use the 80th. It is in the federal registry.”
-
“This is a reasonable percentile based on my experience and use of available comparative resources.”
-
“References recommend using 75-80%. 50% is too low and does not reflect the industry standard especially for specialized providers.”
-
“75th-80 percentile is used by The VA, FairHealth etc. 50th percentile indicates that the evaluee will be excluded from 50% of all service providers in the area.”
Lack of Industry Standard or Authoritative Source Supporting the 80th Percentile
-
“Who says to use 80% v. Other-authoritative source?”
-
“The 80th percentile has been misconstrued to be standard. It is unclear and not documented as to where this came from…”
Percentile Not Available In All Databases
-
“Not databases have data at the 80%ile.”
-
“PMIC is one of the costing resources I use and it does not use 80%.”
-
“I use 75th or 80th, whichever that database uses.”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “50th is the average”
- Response: “not it’s not”
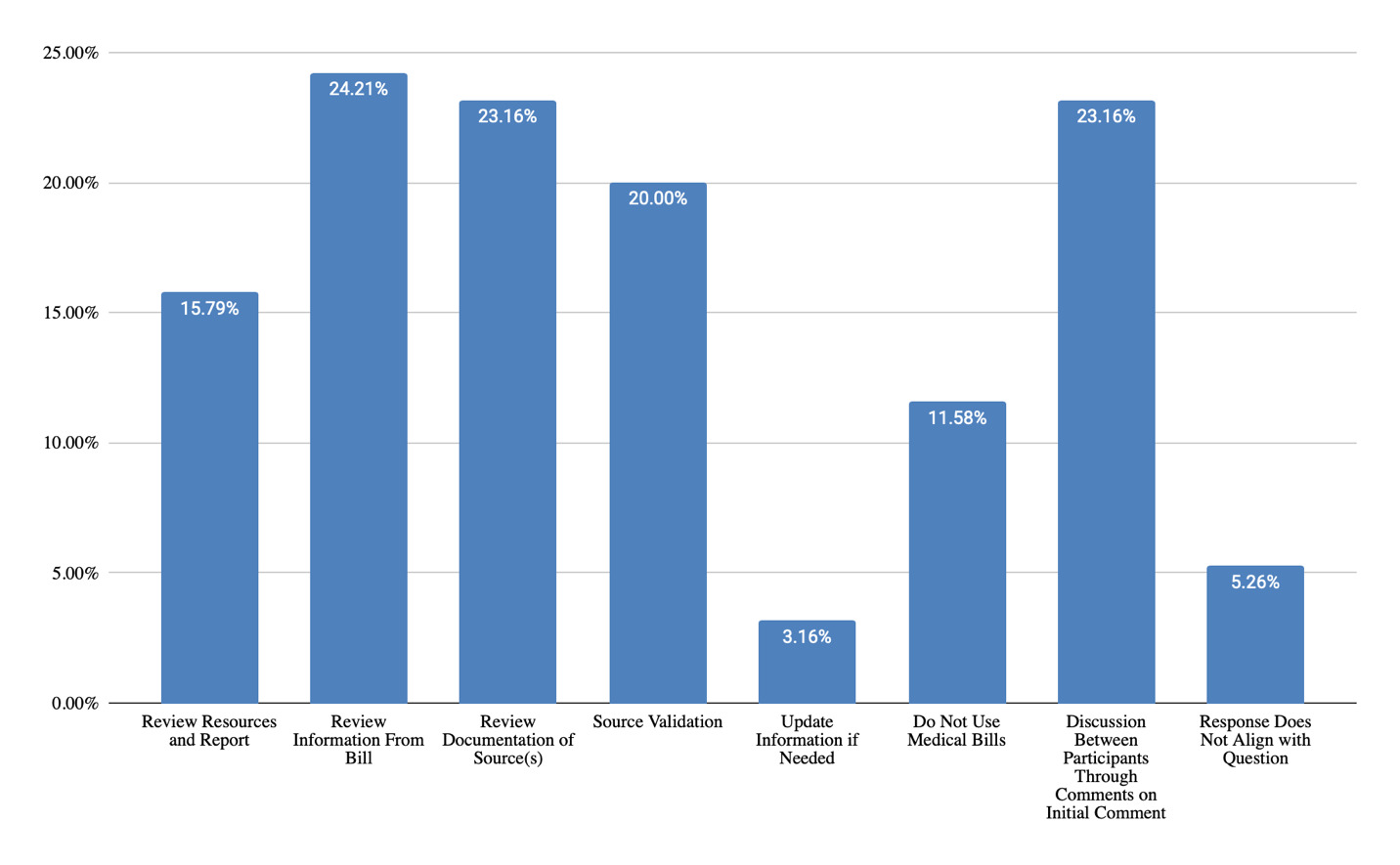
Question 4: “What information do you have prepared regarding medical billing costing techniques before testifying?”
Themes Identified & Representative Examples
Review Resources and Report
-
“Provision of all resources within the report”
-
“Review and understand the information in the file”
-
“Review my costs, numbers, math and resources”
-
“Outlined in my report, review and practice / write down how i might speak to jury in clear language”
Review Information From Bill
-
“I print and highlight the information used, including the CPT codes for those services.”
-
“Take the relevant info from a bill (provider, physician, DOS, charge for service, etc.) and put it on a form to include with my research.”
-
“Codes used, why those codes were chosen, which medical provider recommended those services, geographic area of provider”
-
“Billed amounts, adjustments, payments and balances that remain”
Review Documentation of Source(s)
-
“Documentation of who, what, where, when, specific elements, etc.”
-
“Documentation of source, %, etc”
-
“Source, date, CPT codes used - all pertinent information”
-
“Organize the data, have it ready to describe, have the source of the data, understand how it was obtained.”
Source Validation
-
“Validate my sources, document, validate my foundation”
-
“Data from databases reflecting the parameters 50%-90% to show if billed amount is reasonable.”
-
“Review medical bills and compare with other sources (i.e. calls, databases) by codes”
-
“Organize the data, have it ready to describe, have the source of the data, understand how it was obtained.”
Update Information if Needed
- “…Loo for updates and address appropriately”
Do Not Use Medical Bills
- “Medical bills are in the past and often third party negotiated rates. LCP’s are future…so who cares about the past medical bills while LCP’ing.”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “This is sort of out of contesct, but the attorney gets his 33-40% along with the costs, so the lcp is already underfunded from the get-go. why go with such an minimal approach to medical care in the future?”
-
Response: “Same with expert fees re: Vaccine Compensation Fund”
-
Response: “Attorneys do not always get paid from the settlement (e.g,., Vaccine Compensation Fund)”
-
Response: “expert fees are also a part of those fees.”
-
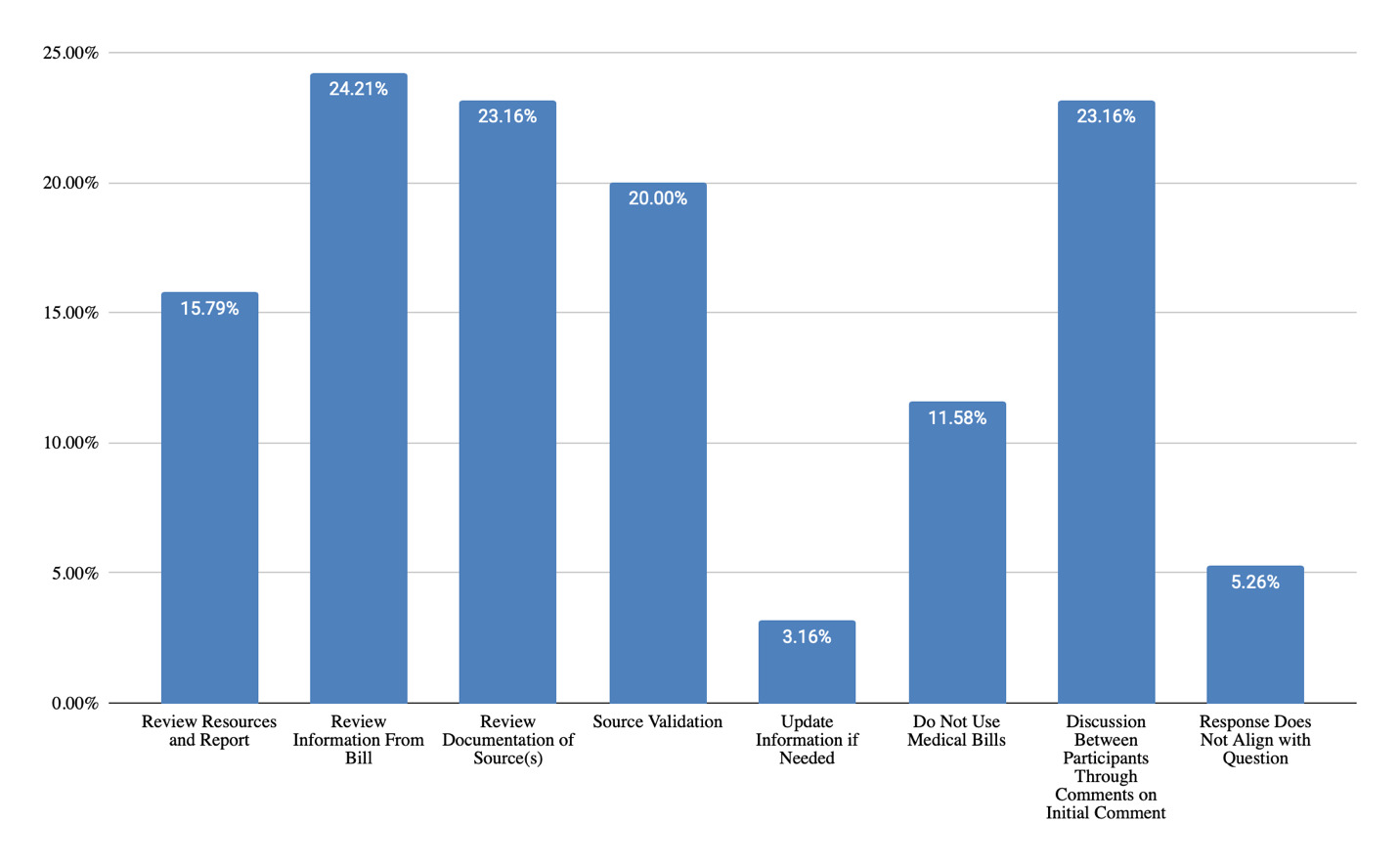
Note. One comment did not align with the question in Figure 14 but was an issue “liked” by 18 people, had four secondary comments, and accounted for 76% of total responses in the “response does not align with question” bar. The comment was “This is sort of out of contesct, but the attorney gets his 33-40% along with the costs, so the lcp is already underfunded from the get-go. why go with such an minimal approach to medical care in the future?”
Questions Received During Testimony
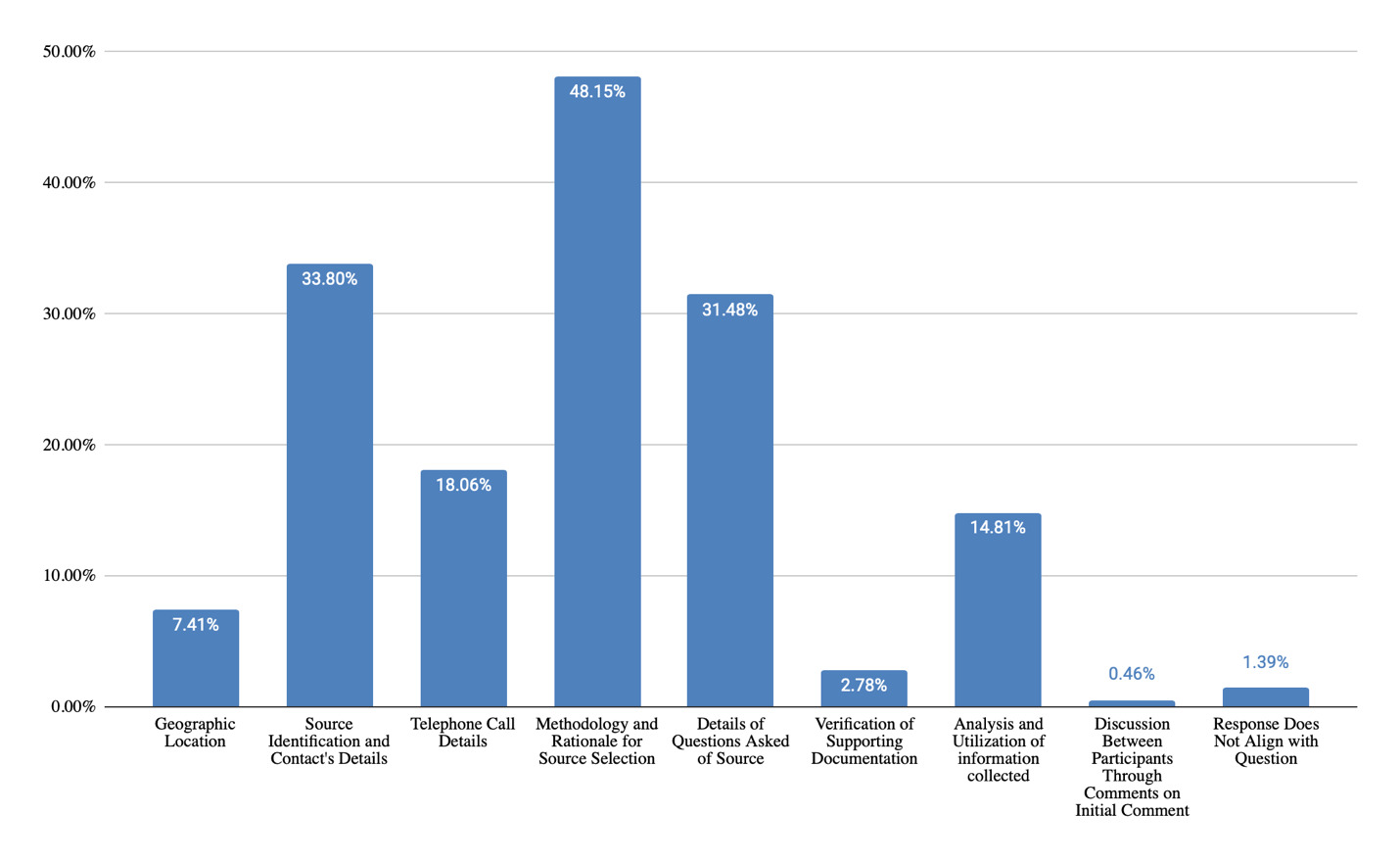
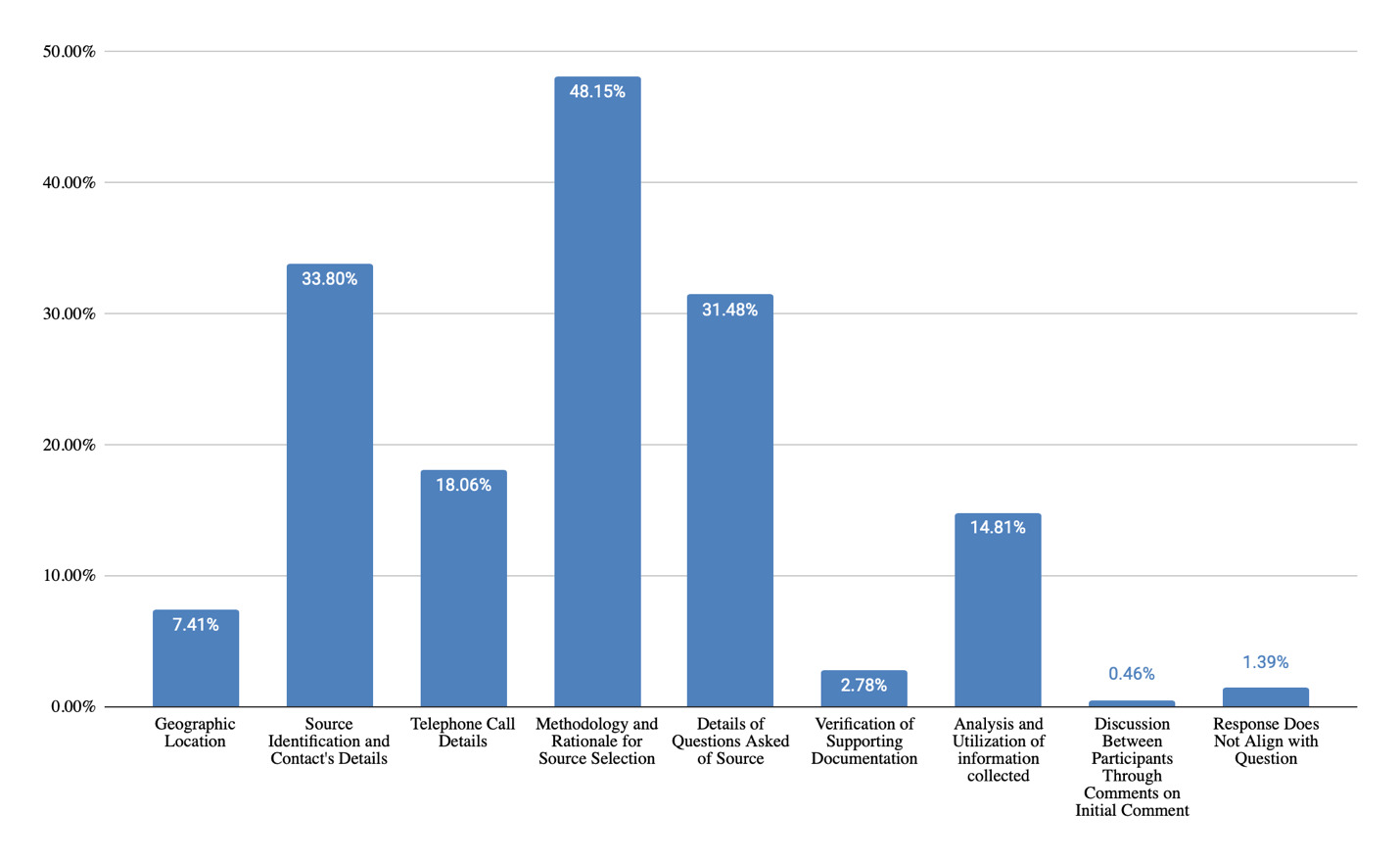
Question 1: “Please describe questions you have received during testimony and how you responded regarding telephone-costing techniques?”
Themes Identified & Representative Examples
Geographic Location
-
“What radius did you use?”
-
" How far away in mileage is the provider from the patient’s home"
Source Identification and Contact’s Details
-
“Who did you talk with? What was their name?”
-
“Who did you call, who did you talk to, what was their position / authority to answer”
-
“Did you make the calls to this vendor? who did you speak to and their title?”
-
“Was he/she qualified to answer your question?”
Telephone Call Details
-
“How recently was this TC done?”
-
“What did you talk about”
-
“How long did you talk?”
-
“Did you make the calls?”
Methodology and Rationale for Source Selection
-
"How did you “randomly” choose three sources? "
-
“Did you pick the most expensive or least expensive providers to get the kind of data you were looking for (plaintiff vs defense cases)”
-
“Why did you make calls to physicians or therapists who were not treating providers in addition to making calls to the treating providers.”
-
“Why did you only call 3 providers, is that representative of the market?”
Details of Questions Asked of Source
-
“Exactly what did you say when you called the home care agency? Did you ask the same question to each one? Do you have a script of what you said? Therefore, I aim to be ready for those questions.”
-
“What did you ask them to obtain the costs?”
-
“What exact words did you use when you spoke to the provider to obtain the fee for service?”
-
“Did you ask for the self-pay price? What questions did you ask? Do you know that is an accurate cost? How do you know?”
-
“Was it a private cost or discounted.”
Verification of Supporting Documentation
-
“Copy of email that verifies info we discussed.”
-
“Do you have the documentation of the phone call? do you back it up with a written communication like email.”
Analysis and Utilization of Information Collected
-
“How has the information affected my report?”
-
“How do you know these are representative costs?”
-
“Why they [the call recipient] had pertinent info.”
-
“Do you know that is an accurate cost? How do you know?”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “Answer: triangulated the cost information with clinical experience”
- Response: “Define triangulation”
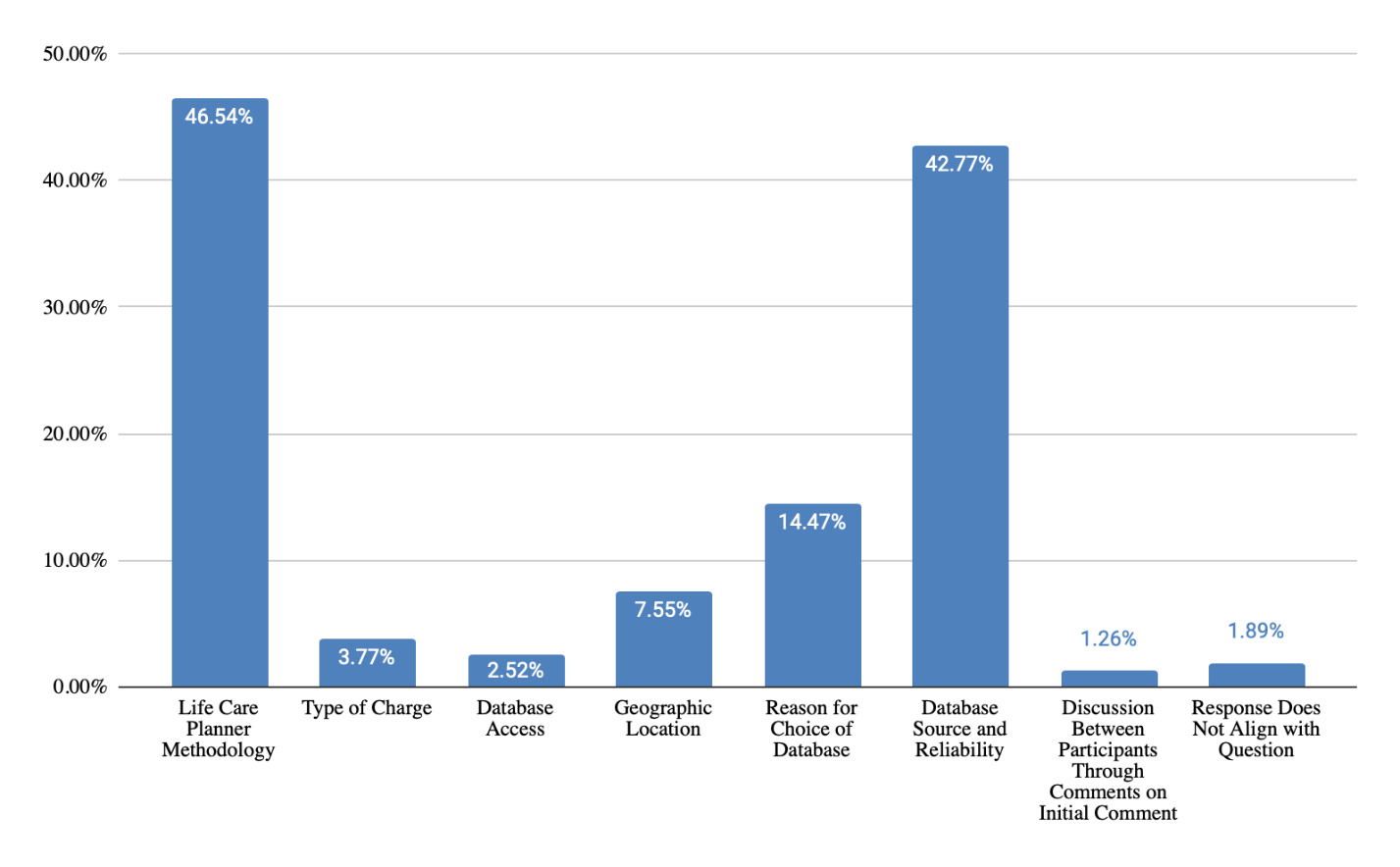
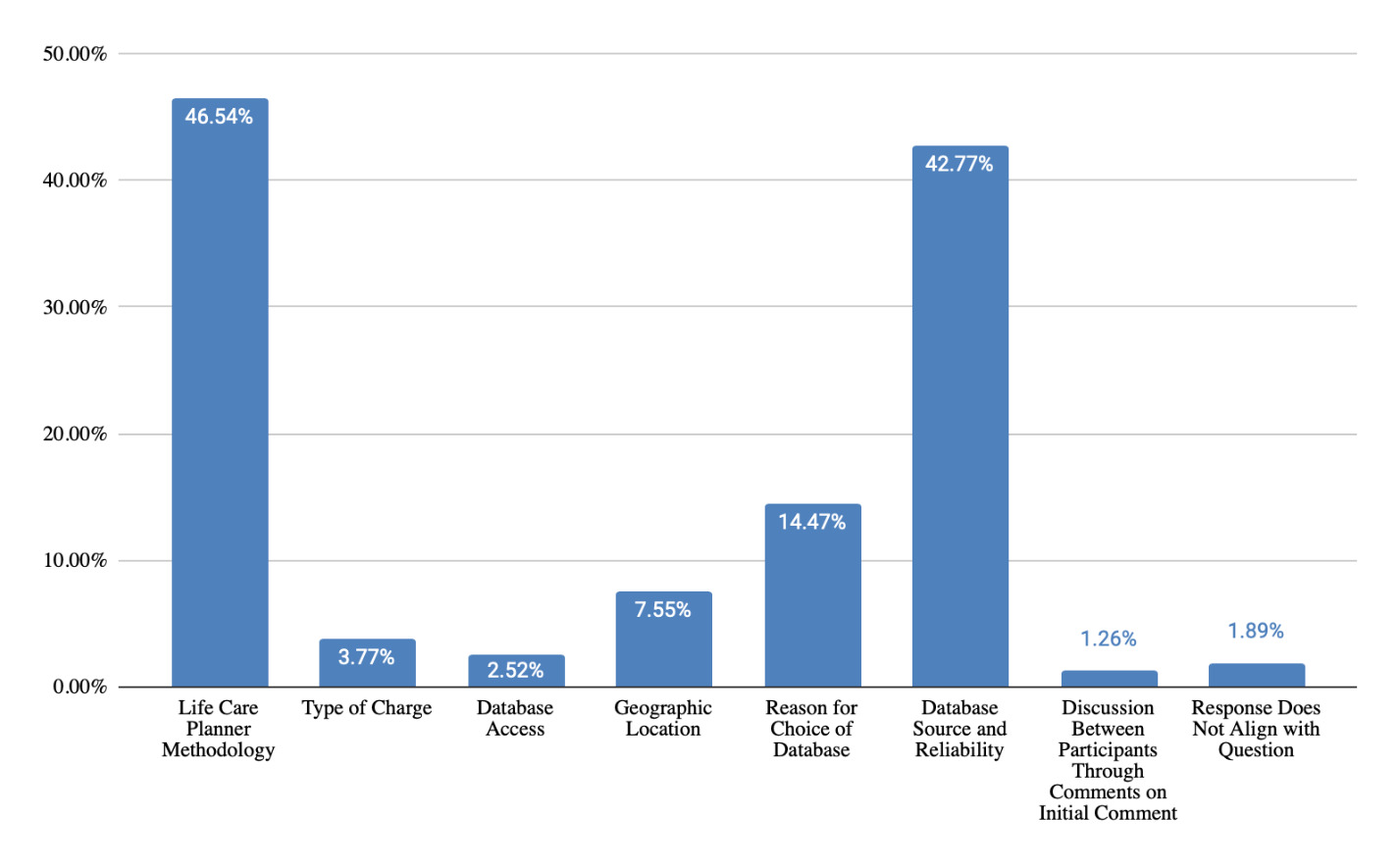
Question 2: “Please describe questions you have received during testimony and how you responded regarding database techniques?”
Themes Identified & Representative Examples
Life Care Planner Methodology
-
“How did you pick which price to use?”
-
“What percentage? What percentile?”
-
“What is your methodology in using databases vs calling 3 providers - AND - where is this in the LCP Standards of Practice.”
-
“What CPT codes did you use?”
-
“What resource did you use? I used the triangulation technique by comparing mulitple sources to determine an accurate fee.”
-
“I was asked specifically about Verci”
Type of Charge
-
“Is it the charge or the inusrance allowable? why is the allowable not relevent? what does medicare pay for that ?”
-
“A lot of questions about… the issue of reimbursement vs. charge rates. there is a lot of misunderstanding about databases NOT being related to insurance/reimbursement rates.”
Database Access
-
“Only you have access, or those who pay for a subscription, correct?”
-
“What is the name of this database? How would I access it?”
Geographic Location
-
“Is this national figures or local?”
-
“How do you adjust geographically?”
-
“Why did you use 75th percentile? Because it gives the patient access to 75% of the providers to choose from and it reflects the charges I gathered from actually calling potential providers in the community the patient lives in.”
-
“Do you know if your evaluee’s doctors costs are in this database? I do not specificially, but this is a representative cost for this service in their geozip.”
Reason for Choice of Database
-
“Why do you use that data base?”
-
“Why did you use that percentile/database?”
-
“Which one do you use”
-
“Why did you use the VA Reasonable Charges data when the evaluee is not a veteran?”
Database Source and Reliability
-
“How do you know this data is reliable?”
-
“Where does the data come from?”
-
“Describe the database and how they obtain their data”
-
“Have you personally seen and analyzed the sources that they use to derive these costs?”
-
“Where did they get their data from? Did you see their raw data? How do you know that what they are reported are true and actual prices? Are these databases created for LCPing or for other purposes? Isn’t it true that these databased are intended to be used for other purposes and that the LCPing community only started using them b/c they are easier even though they are not as accurate”
-
“Where does the database data come from? Isn’t this based on Medicare figures?”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “Why did you use that percentile/database? I triangulate my market research with the database percentiles and use industry accepted database sources”
- Response: “Define triangulate”
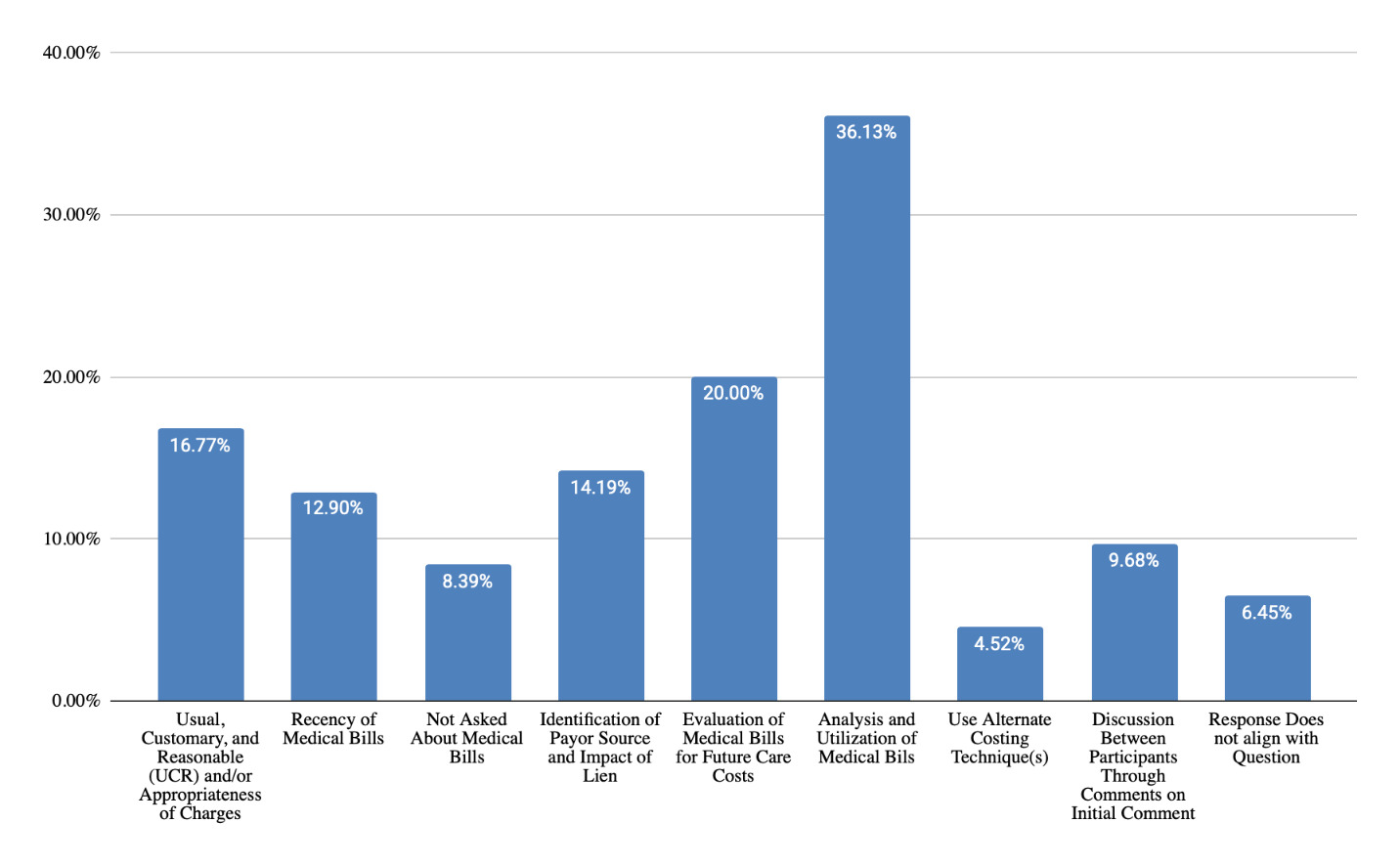
Question 3: “Please describe questions you have received during testimony and how you responded regarding medical billing costing techniques?”
Themes Identified & Representative Examples
Usual, Customary, and Reasonable (UCR) and/or Appropriateness of Charges
-
“How do you know what was billed is a reasonable rate? How old were the bills reviewed. How do you know that is what they will continue to require?”
-
“What exactly is UCR?”
-
“How do you know what is UC?”
Recency of Medical Bills
-
“How old were the bills reviewed. How do you know that is what they will continue to require?”
-
“Did you use the appropriate year of service for comparison”
-
“How far back do you consider bills as a valid cost”
Not Asked About Medical Bills
-
“None”
-
“Not really asked about this”
Identification of Payor Source and Impact of Lien
-
“On lien cases - is the balance due actually due from the patient?”
-
“Where did you get the bills from? Did they come straight from the attorney’s office? Are those attorney costs? do you know who paid those bills and if that full amount was actually paid?”
Evaluation of Medical Bills for Future Care Costs
-
“How do you know that is what they will continue to require?”
-
“Do you use past medical bills to determine costs contained in a lcp”
-
“So, isn’t what has been billed the amount that will be needed on the future?”
Analysis and Utilization of Medical Bills
-
“How do you utilize medical billing?”
-
“I look at them for trends in care, coding, and compare them to the records.”
-
“Have you compared these billings to the actual services provided? Is everything billed related to the incident?”
-
“Why didn’t you use the bills?”
-
“Did you look at medical bills when determining costs in your life care plan”
Use Alternate Costing Technique(s)
- “What is your methodology? I utilize National databases and market research data”
Discussion Between Participants Through Comments on Initial Comment
-
Initial comment: “Soooo what percentile do we leave here using?”
- Response: “For what its worth, US Department of Veterans Administration (VA) using Geographically-adjusted charges and the 80th percentile conversion factors. If VA finds it acceptable for 80, why not use?”
-
Initial comment: “You are not going to testify to the appropriateness of charges are you?”
-
Response: “Is this question for the person in the role as a LCP or a past bill review for reasonableness?”
-
Response: “I ask them to clarify this question- are you asking me to provide a medical opinion- I am only providing an opinion as to the reasonableness of the charges.”
-
Discussion
The purpose of this study was to analyze qualitative data collected through the Top Hat platform during the 2022 Life Care Planning Summit to better understand costing techniques used by life care planners, strengths and challenges associated with each technique, and defense of techniques during testimony. The findings across the 17 focus group questions reveal current costing practices and considerations useful for the development of a costing framework. They can help life care planners make informed decisions when choosing among available costing techniques and strengthen the defensibility of life care plans.
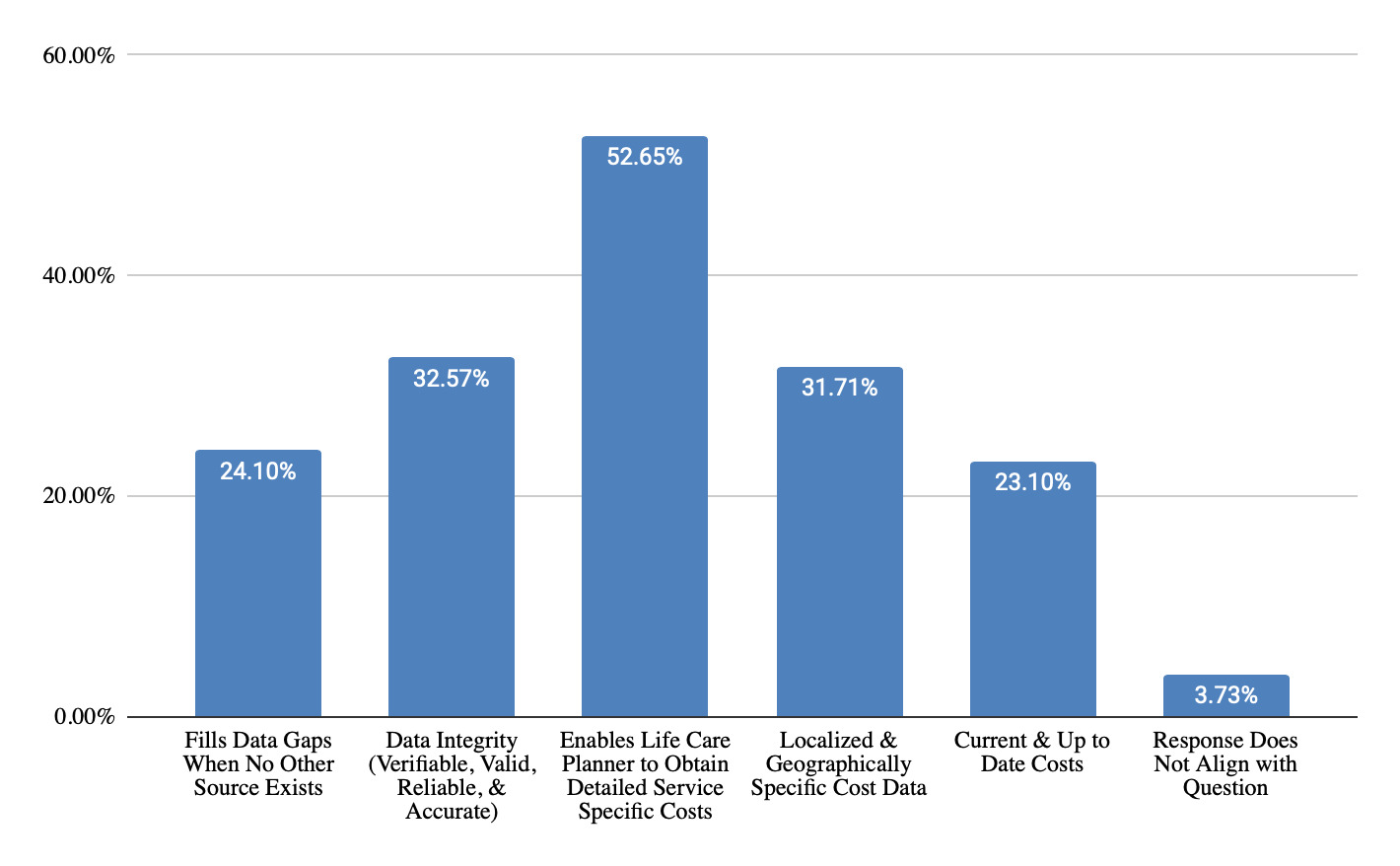
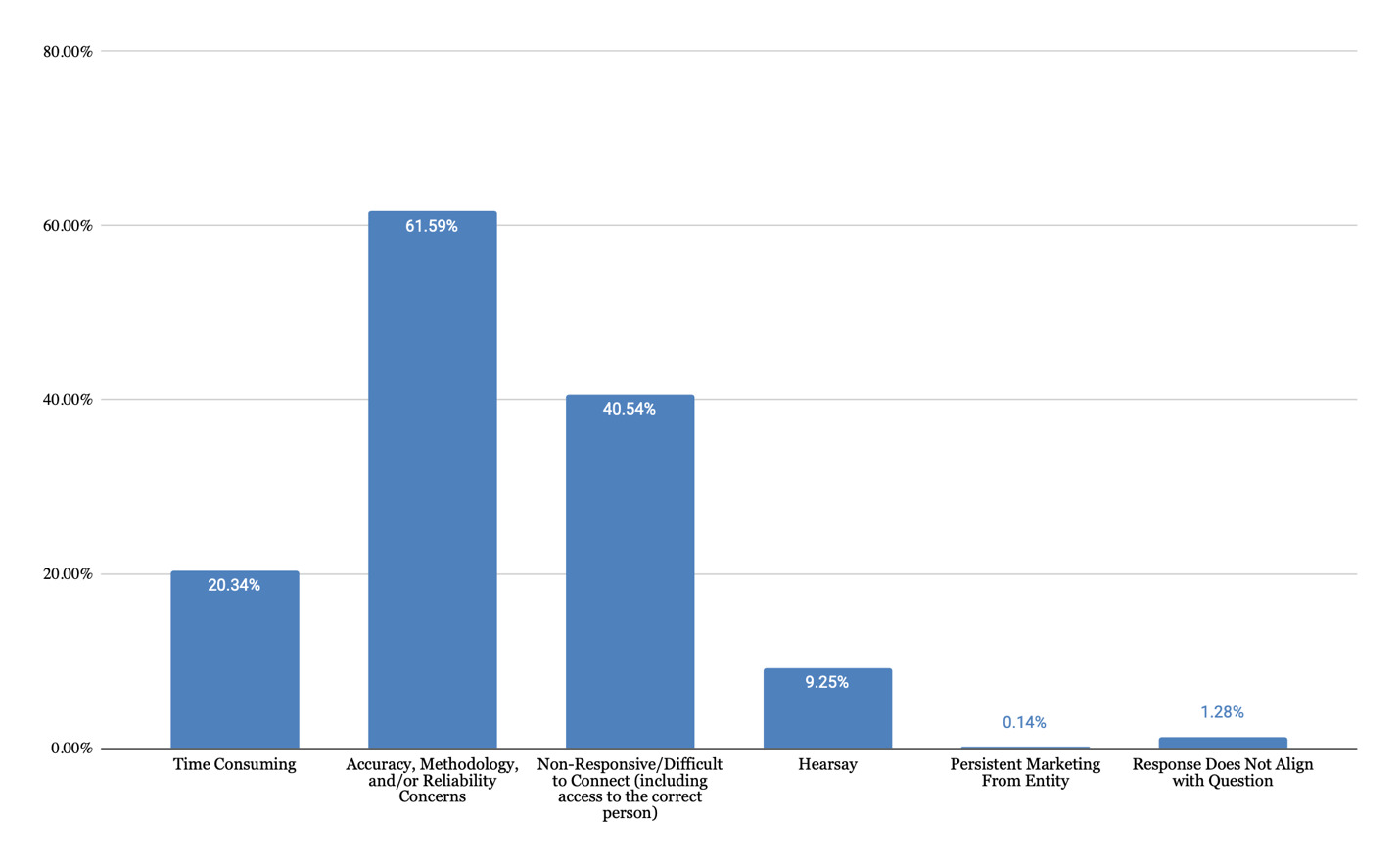
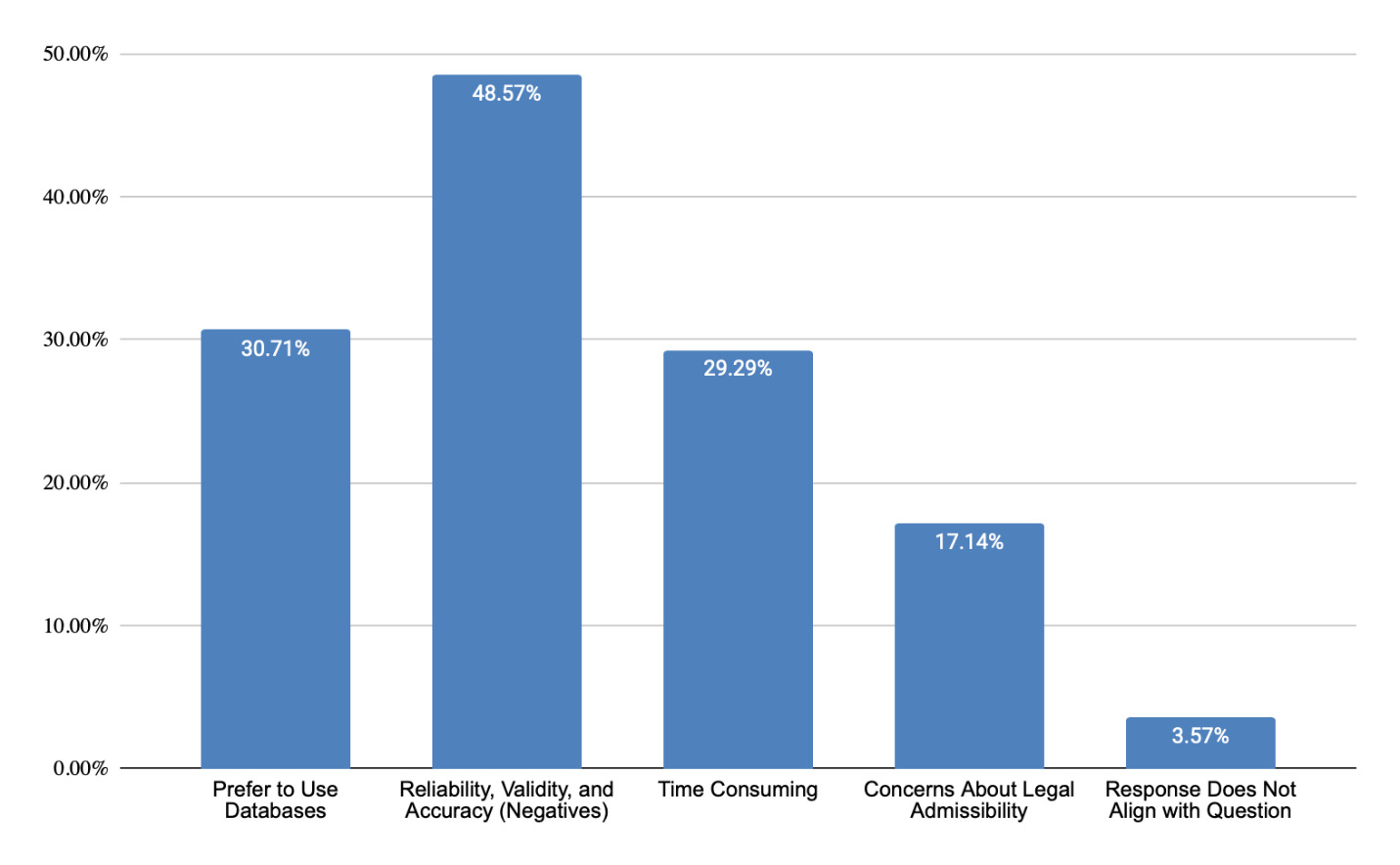
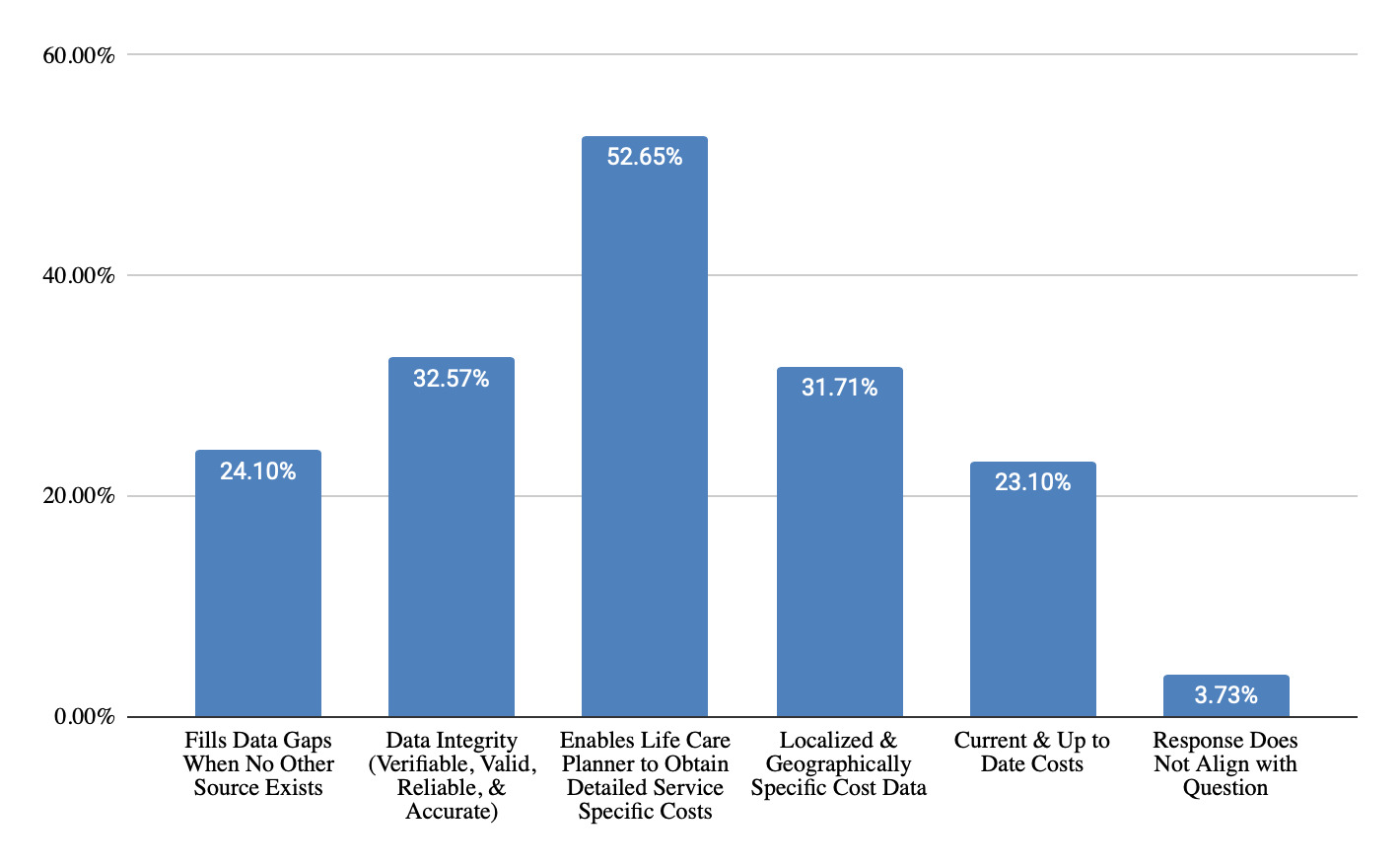
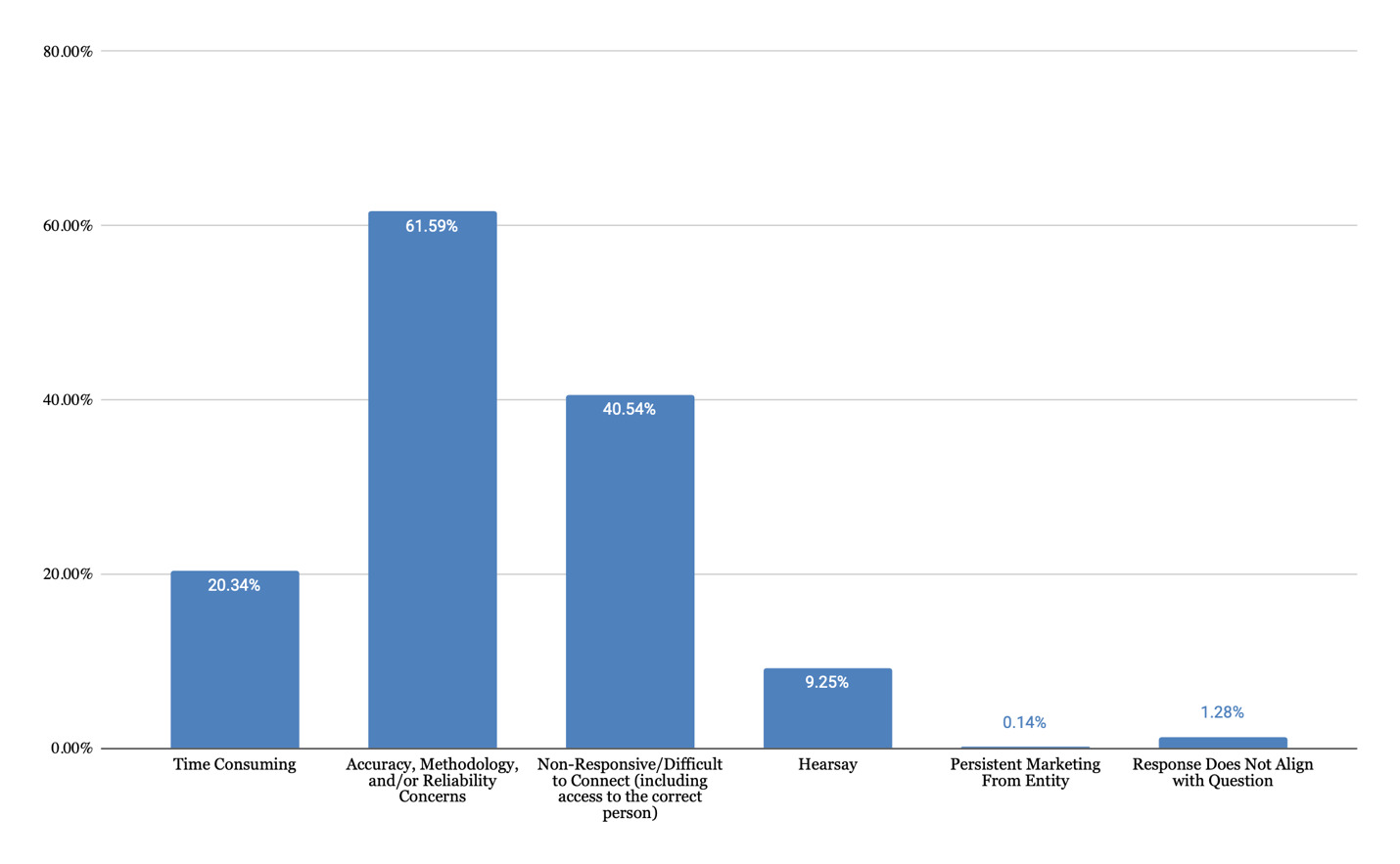
As shown in Figure 1, life care planners value telephone calls for obtaining detailed, service-specific costs (53% of responses) that are geographically-specific (32% of responses) and current (23% of responses). Telephone calls are viewed as verifiable, valid, reliable, and accurate (33% of responses). They fill data gaps when other sources are insufficient (24% of responses). These strengths align with foundational life care planning guidance emphasizing individualized costing. However, time constraints (20% of responses), concerns regarding accuracy and reliability of information (62% of responses), difficulty connecting with the right person (41% of responses), and concerns regarding hearsay (9% of responses) are noted as challenges (Figure 2). Those who do not use telephone calls as a technique (Figure 3) cited a preference for using databases (31% of responses), concerns regarding reliability, validity, and accuracy (49% of responses), time required (29% of responses), and concerns about legal admissibility (17% of responses).
Strengths of using paid databases as a costing technique (Figure 4) were noted to be reliability and reproducibility of data (66% of responses), large sample size (40% of responses), and geographic specificity (16% of responses). These findings align with established consensus statements emphasizing defensible, transparent methodology. However, challenges were also cited (Figure 5), such as lack of transparency in data collection methods (22% of responses), lack of differentiation by provider specialty (20% of responses), subscription cost (17% of responses), complicated and difficult to use (12% of responses), need for proficiency in medical coding (12% of responses), and lack of consensus among life care planners about percentile utilization (7% of responses). Those who do not utilize paid databases (Figure 6) cited reasons being a preference for using a different method of obtaining costs (29% of responses), disagreement with database methodology (24% of responses), cost of databases (10% of responses), uncertainty about how to choose between databases (10% of responses), technological challenges (10% of responses), lack of geographically specific data (10% of responses), and lack of database transparency (10% of responses).
Per Figure 7, medical bills were valued for utilization of coding (54% of responses), showing actual provider charges (51% of responses), being specific to the evaluee (30% of responses), providing information in addition to charges (24% of responses), and for use in triangulation of current data (21% of responses). However, challenges were identified (Figure 8), including potential for limited, incorrect, or unclear information (34% of responses), issues with coding and bundling (31% of responses), concern regarding inflated or discounted charges (31% of responses), data being outdated (23% of responses), and difficulty reading or interpreting the bills (8% of responses).
Free databases were appreciated for being free and accessible (44% of responses), reproducible, verifiable, and credible (43% of responses), and useful for cost comparison (23% of responses), per Figure 9. Some comments reflected endorsement of a specific database (29% of responses). Challenges identified included concern for database methodology, reliability, reproducibility, and transparency (64% of responses), user knowledge, learning curve, and usability (15% of responses), restrictions on use for litigation (15% of responses), and unwanted solicitation after requesting information (12% of responses), per Figure 10.
Per Figure 11, responses regarding information prepared regarding telephone costing before testifying reflected the need for life care planners to review data sources and documentation regarding telephone calls (87% of responses), review methodology used to obtain and document cost information (49% of responses) and make updates to costing research (8% of responses). Information prepared regarding database costing, per Figure 12, included documentation of life care planner methodology (73% of responses), database methodology (49% of responses), review of data gathered (14% of responses), and use of footnotes and citations in the report (9% of responses).
The discussion of the use of specific percentiles showed that 50% of responses indicated agreement with use of the 80th percentile, 42% of responses agreed with use of the 75th percentile, and 8% of responses agreed with use of the 50th percentile, per Figure 13. Nine percent of responses disagreed with use of the 80th percentile, 12% of responses disagreed with use of the 75th percentile, and 8% of responses disagreed with use of the 50th percentile. The rationale behind percentile selection and use of clinical judgement was reflected in 55% of the responses. Forty percent of responses indicated a preference for use of the 80th percentile based on published research, resources, and literature, while 12% of responses indicated there is a lack of industry standard or authoritative source supporting the 80th percentile. Eleven percent of responses mentioned that certain percentiles are not available in all databases.
Information prepared regarding medical billing costing techniques prior to testifying (Figure 14) includes review of information from the bill (24%), review of documentation of sources (23%) validating sources (20%), and reviewing resources used in the report (16%). Twelve percent of responses were in the theme “do not use medical bills.”
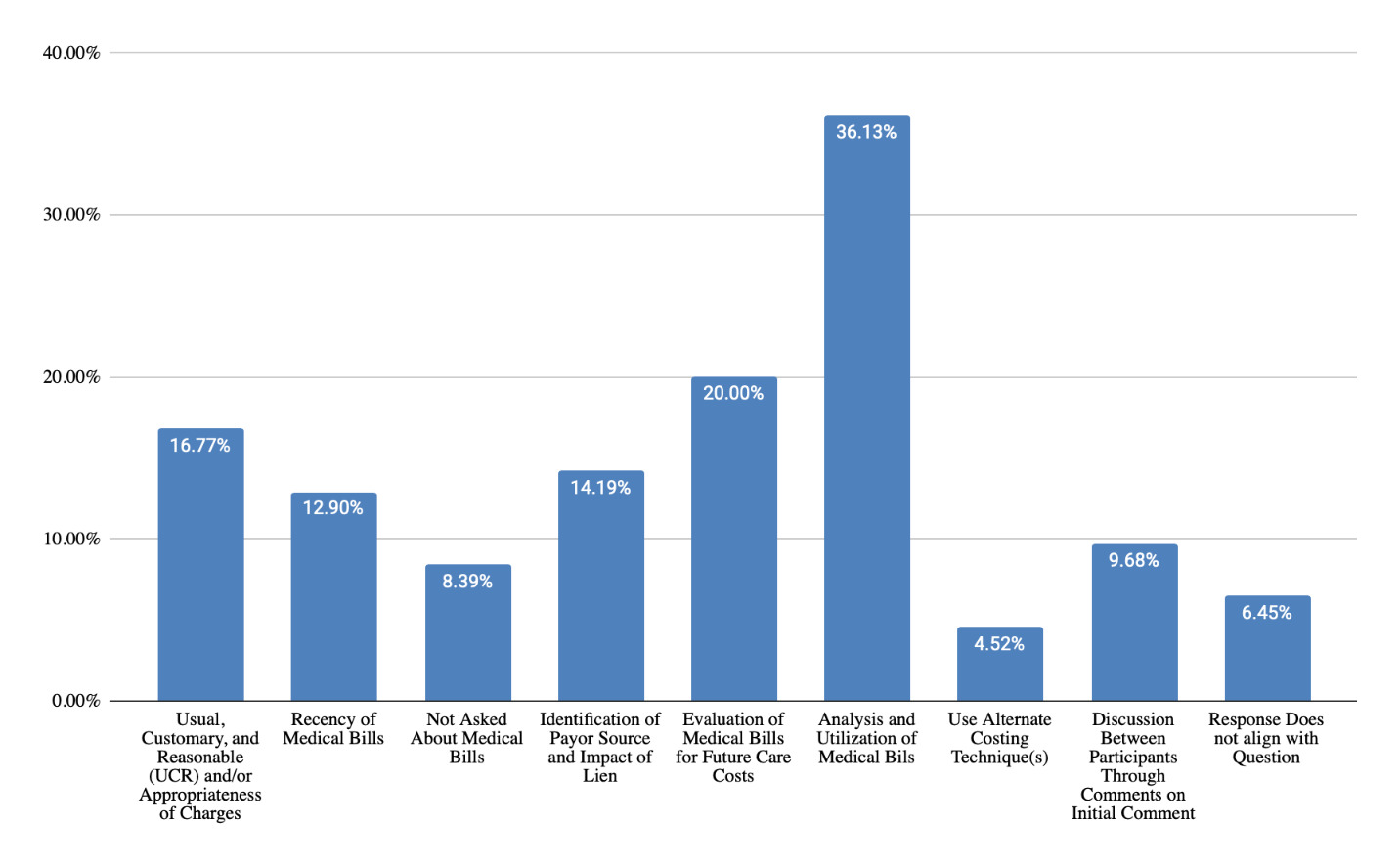
For questions received and responses regarding telephone costing techniques during testimony (Figure 15), themes were clustered around methodology and rationale for source selection (48% of responses), identification of sources and contact’s details (34% of responses), details about questions asked of sources (31% of responses), analysis and utilization of information collected (15% of responses), and geographic location used (7% of responses). Questions and responses regarding database techniques (Figure 16) were grouped into themes including life care planner methodology (47% of responses), source of database data and reliability (43% of responses), and reason for choice of database (14% of responses). For questions and responses regarding medical billing costing techniques, responses included analysis and utilization of medical bills (36% of responses), evaluation of medical bills for future care costs (20% of responses), UCR and appropriateness of charges (17% of responses), identification of payor source and impact of lien (14% of responses), recency of medical bills (13% of responses), and not asked about medical bills (8% of responses).
Limitations
Several limitations were identified regarding data collected through the Top Hat platform. For each question, the number of recorded responses exceeded the number of respondents due to the platform’s “like” feature. As a result, some participants may have “liked” multiple comments, while others may have “liked” only a few or none. Unlike prior summits, attendees were not required to respond to every question. The platform did not allow analysis of how many unique users engaged with each question. Therefore, it was not possible to determine the level of each individual’s active participation within each breakout session.
In addition, a “like” was intended to signal interest in further discussion, not agreement with a comment’s content. It is unclear if participants understood this distinction, given that the use of a “like” often indicates agreement. Many comments contained multiple themes, and it was not possible to determine whether “likes” referred to an entire comment or only part of it. This may have caused certain themes to appear more strongly supported than intended.
The findings from this study represent the perspectives of the life care planners who attended the 2022 Summit and participated in the Top Hat–based focus group sessions. We do not know if these results are representative of the entire community of life care planners without further study. Time constraints necessary to accommodate the overall Summit agenda may have limited the depth of participant responses and discussion. Given more time than the three-minute limit, additional information may have been generated.
Some comments revealed gaps in knowledge and highlighted opportunities for further education. For example, one response to the question on percentile use stated that “50th is the average,” underscoring a need for greater clarity on concepts such as percentile versus percentage and the limitations of averaging percentiles.
Future Research
Information gathered and the conversations generated were deemed to be reliable for the purpose of developing a Costing Framework Tool and may serve as a foundation for future research. We recommend that this study be repeated to facilitate the evolution of the costing framework. If it is repeated, it would be helpful to re-word the questions slightly to generate more specific answers. For example, the questions starting with “Please describe questions you have received during testimony and how you responded” were two-part questions and it was difficult to separate out people’s responses to each part of the question. Also, a separate indicator for agree/disagree is recommended, rather than just an indicator for wanting to discuss a comment further. Desire for engagement does not necessarily indicate agreement. Other methods of costing which were not addressed in this survey could be researched in the future, such as the use of chargemasters. Price transparency federal rules were initiated in 2021 but were not consistently implemented by hospitals until after the Top Hat survey questions were developed; therefore, chargemasters were not addressed.
Conclusion
This qualitative analysis of Top Hat responses from the 2022 Life Care Planning Summit provides insight into costing practices, methodological decision-making, and testimony preparation within the field of life care planning. Life care planners rely on a combination of data sources, including telephone calls, paid databases, medical bills, and free/open-access resources, each serving a distinct role depending on context and purpose. The themes identified in this analysis emphasize the role of life care planners as analysts who must select the most appropriate techniques for each costing situation. Although variability exists, most notably in percentile selection, the findings demonstrate shared values including accuracy, reliability, reproducibility, transparency, defensibility, and methodological consistency. The themes identified through this qualitative analysis are consistent with foundational documents published on life care planning costing methodology (see Chapter 1). The findings can help life care planners make informed decisions when choosing among available costing techniques and strengthen the defensibility of life care plans. The results of this analysis contribute to the development of a Costing Framework Tool.